

Ebola Is Back. And This Time We Are Less Ready.
Funding for CDC and WHO cut dramatically and it counts

The virus never disappeared. Our attention did.
Just when you think we can relax from a viral epidemic: Ebola.
The Democratic Republic of Congo confirmed another Ebola outbreak. Current estimates suggest roughly 246 suspected infections and at least 65 deaths. Early sequencing suggests this may not be the classic Zaire strain — the one for which we already have an approved vaccine. That matters. A great deal.
Because Ebola is not just another “bad flu.” It is one of the most lethal viruses modern medicine encounters. Depending on the strain, mortality can range from 25% to nearly 90%.
And yet what struck me reading the reports was not merely the outbreak itself. It was the uneasy realization that ten years ago, we were far more prepared for this moment than we are now.
During the West African Ebola epidemic of 2014–2016, the United States anticipated that Ebola could reach our shores. Public health agencies trained hospitals. Isolation units were prepared. Airports screened passengers. The CDC mobilized rapidly. Scientists collaborated internationally. The military assisted with logistics. The WHO coordinated surveillance.
I was chairman of surgery at the time, and we had meetings about Ebola. We were told to expect Ebola in the United States. We put protocols in place, had isolation rooms ready. We taught signs and symptoms and had PPE gear ready and stored for when Ebola hit our shores. The reason it didn’t was because of the intervention we did through WHO and the CDC that kept Ebola in Africa. We did bring home several Americans infected, but not contagious.
There was anxiety, certainly. But there was also infrastructure.
Today we have something very different: exhaustion, fragmentation, and political contempt for public health itself.
We cut expertise and then congratulate ourselves for “saving money.” We withdrew from international partnerships and then pretend viruses require passports. We lost experienced personnel from the CDC and global surveillance networks precisely as the world became more interconnected than at any point in human history.
Viruses do not care about ideology. Ebola certainly does not.
What Ebola Actually Is
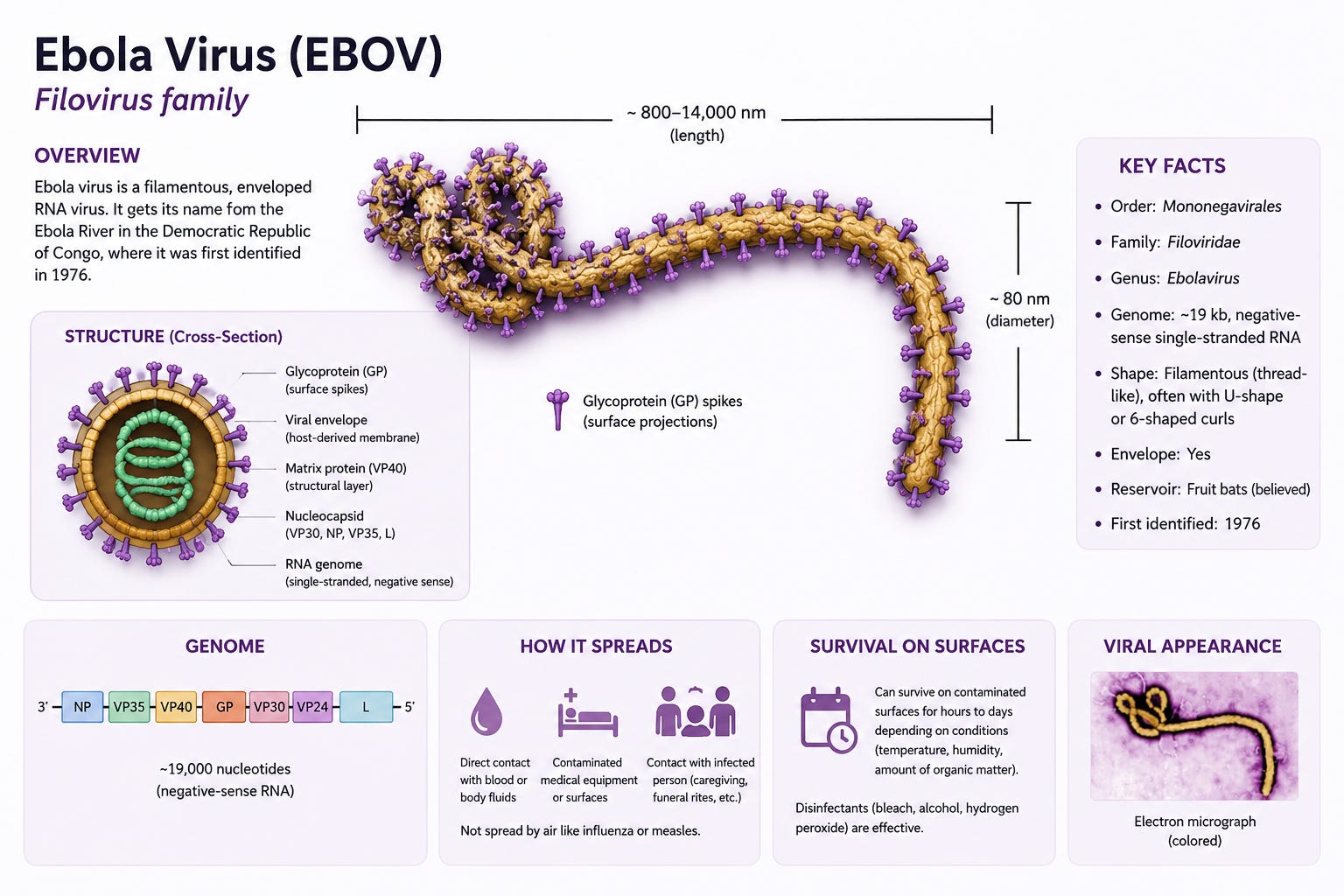
Ebola is caused by a filovirus — a long, filament-shaped RNA virus. Unlike DNA viruses, RNA viruses mutate relatively quickly. They are sloppy copiers. That biological chaos is part of why outbreaks can evolve unpredictably.
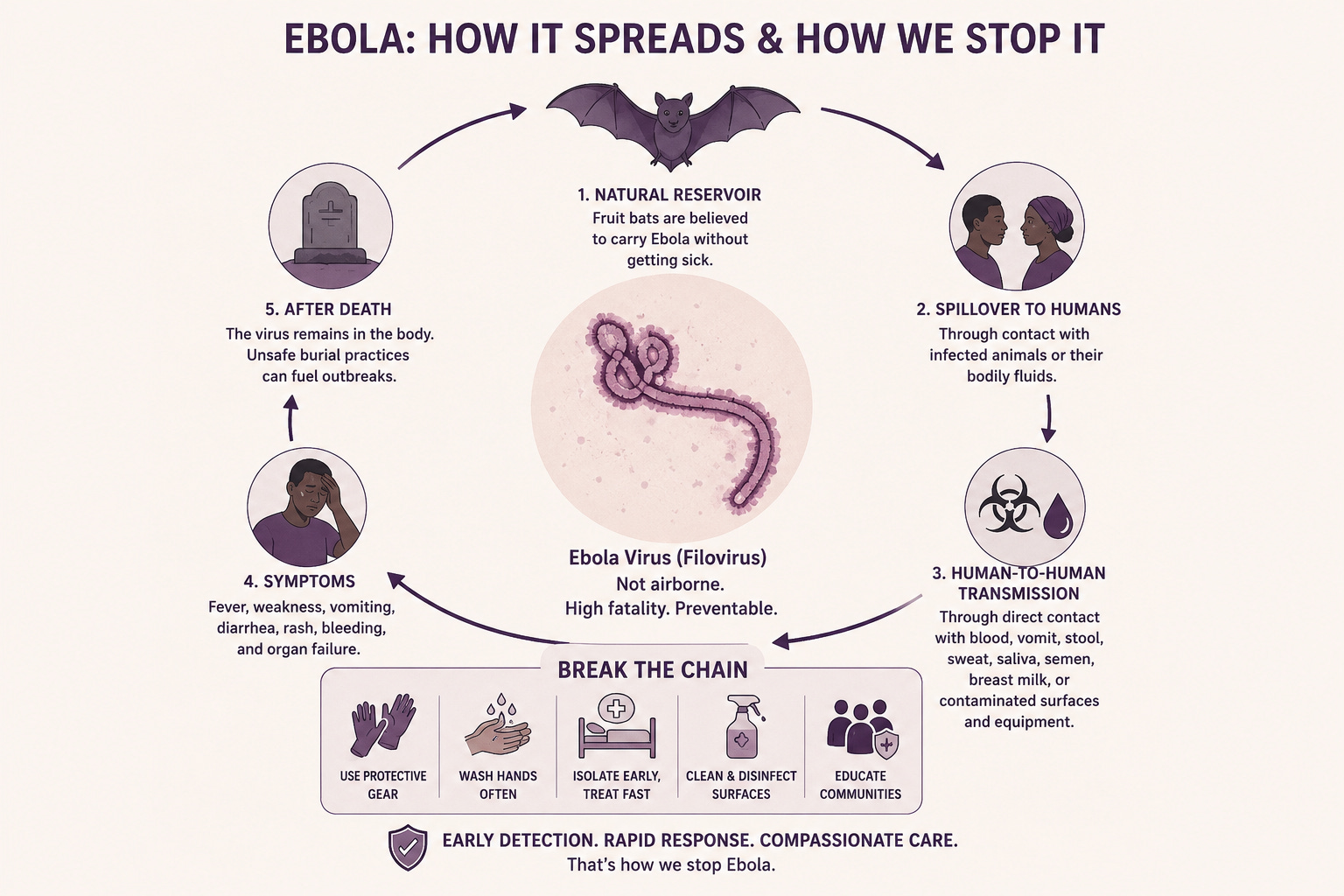
The natural reservoir is believed to be fruit bats. Humans usually become infected through contact with infected animals or contaminated bodily fluids from infected individuals.
And this is important: Ebola is not airborne in the way measles or COVID can be.
It spreads primarily through direct contact with blood, vomit, stool, sweat, saliva, semen, breast milk, and contaminated surfaces or medical equipment. Caregivers and healthcare workers are at particular risk when protective systems fail.
That distinction matters, because it means Ebola is both terrifying and containable — if you have functioning public health systems.
The virus causes fever, weakness, vomiting, diarrhea, rash, and in severe cases, bleeding and organ failure. The immune system becomes overwhelmed. Blood vessels leak. Clotting systems collapse.
It is a brutal disease.
And unlike many respiratory viruses, Ebola can persist in survivors long after recovery. The virus has been detected months later in semen, ocular fluid, and even the central nervous system. Survivors may clear symptoms, yet still harbor reservoirs of infection.
That is one reason outbreaks can reignite unexpectedly.
What We Did Last Time — And Why It Worked

During the major West African Ebola outbreak, the world did not simply sit back and hope for the best.
The United States deployed CDC teams directly into outbreak zones. Epidemiologists tracked chains of transmission village by village, patient by patient. Mobile laboratories were established so that viral testing could occur in hours instead of weeks. Military logistics teams helped move supplies, personnel, and protective equipment into areas with almost no infrastructure.
Field hospitals and specialized Ebola treatment units were rapidly constructed. Healthcare workers were trained in infection-control procedures that most hospitals in the developed world take for granted, but are extraordinarily difficult to implement in resource-poor settings, wearing layers of suffocating protective gear in tropical heat.
And then came one of the hardest realities: burial practices.
Ebola remains highly infectious after death. Traditional funeral rituals involving washing and touching the body became major amplifiers of spread. International teams worked with local communities to establish safe burial protocols that still respected cultural traditions, while preventing further transmission.
That meant trained mortuary teams. It meant protective equipment. It meant vehicles, refrigeration, disinfectants, and personnel willing to do emotionally devastating work under dangerous conditions.
At the same time, the World Health Organization coordinated international surveillance, funding, and communication between countries. Wealthier nations provided emergency resources because everyone understood a simple truth: stopping Ebola in central Africa was far cheaper — and far safer — than allowing it to spread internationally.
This was not charity. It was intelligent self-defense.
And that is the part many people forget.
Public health only looks “expensive” until you compare it with the cost of failure.
Today, many of those systems are weaker. Funding has been reduced. International partnerships have frayed. Experienced personnel have left. Support for WHO coordination has become politically controversial. Outbreak preparedness has increasingly been treated not as national security, but as optional bureaucracy.
Viruses exploit exactly that kind of complacency.
What Has Changed Since The Last Ebola Crisis
During the last major Ebola response, the United States was the logistical backbone of global outbreak containment.
Today, that backbone is weaker.
The United States formally completed its withdrawal from the World Health Organization after halting funding and pulling personnel from WHO operations. The U.S. had historically been WHO’s single largest contributor, providing roughly 15% of the organization’s budget — hundreds of millions of dollars annually that funded outbreak surveillance, laboratory support, emergency response teams, vaccination campaigns, and field coordination in low-resource nations.
That funding mattered.
WHO is not simply a building in Geneva issuing press releases. It coordinates disease reporting between nations, deploys emergency teams, organizes vaccine campaigns, tracks outbreaks in real time, and helps fragile countries respond before local epidemics become international crises.
At the same time, the CDC itself has undergone significant contraction.
Recent reports estimate the CDC has lost more than 3,000 employees — roughly a quarter of its workforce — during the current administration’s reductions and reorganizations. Proposed federal budgets would reduce CDC funding by more than 50%, while cutting staff by over 40%.
And these are not abstract bureaucratic positions.
The cuts have affected global health units, outbreak analytics teams, disease detectives in the Epidemic Intelligence Service, surveillance specialists, laboratory personnel, and experts who historically deployed to outbreaks involving Ebola, Marburg, mpox, measles, and hantavirus.
During the previous Ebola crises, CDC teams traveled directly into outbreak zones. American experts helped establish field hospitals, train healthcare workers, set up mobile labs, trace contacts, and coordinate safe burial practices.
That response infrastructure is now diminished.
The danger is not merely that another Ebola case could appear. The danger is delay. Delay in detection. Delay in sequencing. Delay in reporting. Delay in deploying trained personnel before chains of transmission expand.
Outbreaks are controlled in the first days and weeks. Once exponential spread begins, medicine becomes far more difficult and far more expensive.
And perhaps the most dangerous change is psychological.
After COVID, much of the political world stopped treating preparedness as essential infrastructure and began treating it as unnecessary overhead. Public health workers became targets, not assets. International cooperation became politically toxic. Expertise itself became suspect.
But viruses do not negotiate with ideology.
Nature does not care whether a government believes in public health. Ebola will replicate perfectly well regardless of who wins an election.
And that is the uncomfortable truth beneath all this: we are entering a more dangerous biological era with fewer defenses than before.
The Lesson We Refuse To Learn
Every outbreak follows the same emotional cycle.
First comes denial.
Then comes mockery of experts.
Then comes sudden panic.
Then comes revisionist history, where everyone claims they “always knew” it was serious.
COVID should have taught us humility. Instead, it taught many people arrogance. They emerged from a once-in-a-century pandemic convinced not that preparedness matters, but that preparedness itself was somehow the enemy.
That is madness.
The world is getting smaller. More humans are traveling into remote ecosystems. More forests are being disrupted. More animal reservoirs are being encountered. More viruses are crossing species barriers.
The next pandemic will not politely announce itself on cable news before arriving.
And the cruel irony is that the systems required to stop outbreaks early are relatively inexpensive compared with the cost of uncontrolled spread. We casually approve trillion-dollar defense budgets, while hollowing out institutions that defend us from organisms we cannot bomb, sanction, or negotiate with.
A virus needs no navy. It only needs an opening.
