

Knowledge Is Not the Problem
What fifty years of obesity research actually tells us

This week, a gym bro told people that we know the answer to losing weight and keeping it off - and oddly, he sells the solution. He was shaming people who take GLP-1 medicines. Stating if they just followed his program they wouldn’ t need a GLP-1 He was wrong - and actually thought he knew the literature - he doesn’t.
The Weight-Loss Advice Paradox
Here is the uncomfortable truth: we have known for decades what successful people do to lose weight and keep it off.
They exercise regularly. They monitor their weight. They pay attention to calories. They limit highly processed foods. They remain vigilant year after year.
So why are we still struggling with obesity?
Before we dive into the literature, let me give you the bottom line:
We know how to lose weight.
What we have struggled with is helping people sustain that weight loss.
Those are two very different questions.
Losing weight and maintaining weight loss are not the same biological challenge. Most weight-loss discussions blur those two together, which is one reason so many people become frustrated. They lose weight, regain it, and conclude they failed. In reality, they successfully solved the first problem and encountered the second.
The arrival of GLP-1 medications has forced us to reconsider an uncomfortable possibility: perhaps the problem was never a lack of information. Perhaps the problem was biology.
Consider elite distance runners. We know exactly how Olympic 5,000-meter champions train. Their workouts are not secret. Their diets are not secret. Their recovery strategies are not secret. We can publish every detail of their training plan online.
Yet almost none of us will ever become Olympic champions by copying their routine.
The reason is simple: success requires more than knowledge. It also requires biology.
Weight loss is similar. We know what successful maintainers do. Researchers have studied them for decades. We can describe their habits in extraordinary detail.
The question is not whether those habits work. In fact, I would think many of my patients who eventually had weight loss surgery did the things that successful people do - seriously, read on.
The question is why so few people can sustain them for years while constantly fighting hunger, cravings, food thoughts, and the body’s powerful drive to regain lost weight.
That question directly takes us into the science of obesity, weight regain, and why the GLP-1 era may have changed everything.
The Most Dangerous Weight-Loss Myth: That If You Knew Better, You’d Do Better
It sounds reasonable, doesn’t it? If people knew how to lose weight, they would lose weight. If they knew how to keep it off, they would keep it off. Obesity, therefore, becomes a problem of information. Find the right information, teach it to enough people, and the problem is solved.
The idea is appealing because it is simple. It also contains a subtle form of circular reasoning. If successful people know what to do, and unsuccessful people do not achieve the same results, then the explanation must be that the unsuccessful people lacked the right knowledge, failed to apply it correctly, or did not remain disciplined enough to continue. The conclusion is built into the premise.
The difficulty with this argument is that we have spent decades studying successful weight-loss maintainers. Researchers have interviewed them, followed them, measured their activity, analyzed their diets, and catalogued their habits. We know a lot about what they do. They exercise regularly, monitor their weight, maintain awareness of their food intake, and continue these behaviors for years. There is very little mystery about the habits associated with long-term success.
Yet obesity remains common. If knowledge alone were the solution, this should not be the case. We would expect the problem to have diminished as nutritional information, exercise science, and public health messaging became more widespread. Instead, obesity rates rose, while information became increasingly available.
When I hear someone claim the answer is already known, and that people simply need to follow the program, there is often a business model attached. Sometimes it is a coaching service. Sometimes it is a workout plan, an app, a supplement line, hormone replacement therapy, or a subscription community. The details change, but the message remains remarkably consistent: the answer already exists, and success is available to anyone willing to follow the system.
The appeal of this message is obvious. It places control entirely in the hands of the individual. If the program works, the program deserves the credit. If it does not work, the individual assumes the blame. The advice remains unchallenged, because failure is attributed to the person, not to the limitations of the intervention.
Obesity researchers, however, have spent years asking a different question. Rather than focusing exclusively on the people who succeed, they have examined what happens across entire populations to lose weight and maintain that loss. Their findings reveal something important: the challenge is not simply losing weight. The challenge is maintaining weight loss in the face of biological systems that actively resist it.
That distinction changes everything. It shifts the discussion away from whether people know what to do, and toward a more important question: why is it so difficult for so many people to continue doing it year after year? The answer is where the modern science of obesity begins.
We Know What Successful People Do
At this point, someone usually responds, “But we know exactly what people do who lose weight and keep it off.”
That statement is true.
One of the most frequently cited sources is the National Weight Control Registry, a long-running project that follows individuals who have successfully maintained substantial weight loss. To qualify, participants must have lost at least 30 pounds and maintained that loss for at least one year. Researchers have studied thousands of these individuals to understand what separates long-term maintainers from everyone else.
The findings are remarkably consistent. Successful maintainers tend to exercise regularly, often for about an hour a day. They monitor their weight frequently. They maintain awareness of what they eat. They limit highly processed foods and continue these behaviors year after year.
These observations are useful. They tell us that long-term weight maintenance is possible. They also tell us what success looks like.
What they do not tell us is how many people attempted the same behaviors and failed to achieve the same outcome.
This is a classic example of survivor bias. During World War II, analysts examined returning bombers to determine where additional armor should be placed. The obvious conclusion was to reinforce the areas with the most bullet holes. Statistician Abraham Wald pointed out the flaw. The planes being studied survived. The missing information came from the aircraft that never returned. The areas without bullet holes were often the places where damage had been fatal.
The same caution applies when interpreting studies of successful weight-loss maintainers. We are examining the people who made it back. We are not examining the far more individuals who adopted many of the same habits, but were unable to sustain the weight loss.
This does not mean the behaviors are unimportant. It means that observing successful people does not automatically reveal the probability of success for everyone else.
Imagine studying Olympic marathon runners and concluding that anyone can become an elite athlete by following the same training plan. The training clearly matters. But so do genetics, physiology, injury resistance, recovery capacity, opportunity, and many other factors. Looking only at the winners tells us something important, but it does not tell us everything.
The same is true in obesity. We know what successful maintainers do. The question is why so many people who understand those behaviors, attempt those behaviors, and often succeed temporarily are unable to maintain them over the long term.
To answer that question, we need to move beyond registries of successful individuals and look at what happens when thousands of ordinary people are given intensive lifestyle interventions and followed for years. Fortunately, we have exactly that study.
The Best Lifestyle Trial Ever Conducted
If the National Weight Control Registry tells us what success looks like, Look AHEAD tells us how often success occurs when we apply those principles to a large population.
Look AHEAD, which stands for Action for Health in Diabetes, enrolled more than 5,000 adults with overweight or obesity and type 2 diabetes. This was not a fad diet, a social media challenge, or a fitness influencer’s coaching program. It was one of the most ambitious lifestyle intervention trials ever conducted.
Participants in the intensive lifestyle intervention group received far more than the standard advice to “eat less and move more.” They were given calorie targets, physical activity goals, meal replacements, behavioral counseling, frequent follow-up visits, and ongoing support from trained professionals. In many ways, it represented the best version of what lifestyle medicine can offer.
The results were impressive—at first.
After one year, participants lost an average of 8.6% of their body weight. For many clinicians, that would be considered a successful outcome. Blood sugar improved. Blood pressure improved. Fitness improved. Many participants experienced meaningful health benefits.
If the study had ended after one year, it would likely be cited today as proof that obesity can be solved through lifestyle intervention alone.
But the investigators kept following the participants.
At four years, the average weight loss had fallen to 4.7%.
At ten years, participants maintained an average weight loss of approximately 6%.
That number deserves careful attention. These were not people who lacked information. They were not people who had failed to receive coaching. They were not people who had ignored professional guidance. They had access to resources and support that most patients never receive in routine clinical practice.
Yet the body pushed back.
Hunger returned. Weight returned. Some participants maintained substantial weight loss, but many regained part or most of what they had lost. The challenge was no longer knowing what to do. The challenge was to continue to do it while fighting powerful biological signals, encouraging weight regain.
Importantly, Look AHEAD was not a failure. Participants experienced improvements in fitness, blood sugar control, quality of life, and several important health outcomes. The lesson is not that lifestyle intervention does not work.
The lesson is that losing weight and maintaining weight loss are different biological problems.
The first problem can often be solved with information, motivation, and support.
The second problem requires overcoming a body that increasingly behaves as though weight loss is a threat that must be corrected.
That realization helps explain why obesity researchers became so interested in treatments that affect hunger, satiety, and energy regulation. The question was no longer whether people knew what to do. The question was how to help them continue doing it after the initial weight loss.
The arrival of GLP-1 therapies would provide the first large-scale test of that idea.
Your Body Has a Thermostat
One way to think about obesity is to imagine your home thermostat.
Suppose it is a hot summer day (or Tuesday if you live in Arizona), and your air conditioner is set to 72 degrees. You decide to open all the windows. Hot air pours into the house. The air conditioner works harder. The system compensates. Eventually, despite the open windows, the house drifts back toward the temperature set by the thermostat.
The opposite happens in winter. Open the windows, and cold air rushes in. The furnace responds by working harder to restore the temperature it has been programmed to maintain.
Body weight appears to work in a remarkably similar way.
When people lose weight, the body does not simply congratulate them and continue operating normally. Instead, a series of biological responses are activated. Hunger increases. Satiety signals weaken. Food becomes more rewarding. Energy expenditure often falls. The body begins to behaving as though it is trying to restore the weight lost.
This is not a failure of character. It is a feature of human physiology.
For decades, obesity researchers have referred to this concept as a defended body weight or body-weight set point. While the exact mechanisms are complex and still being studied, the observation is remarkably consistent: the body frequently treats weight loss as a deviation from its preferred state and activates systems designed to reverse it.
That is what Look AHEAD demonstrated. Participants knew what to do. They received coaching, support, education, meal plans, and follow-up. Many lost significant weight. Yet over time, biology began pushing back.
The question is not whether people can temporarily overpower the thermostat. Many can.
The question is how long they can continue fighting a system designed to restore the previous setting.
For some individuals, extraordinary effort is enough. They become the success stories we celebrate and study. For many others, maintaining that effort year after year becomes increasingly difficult as hunger, cravings, and food thoughts return.
This is where GLP-1 medications become interesting. Rather than asking patients to overpower the thermostat through willpower alone, these medications appear to influence the systems that regulate hunger, satiety, and energy balance.
In other words, they do not simply help people do the right thing. They help change the biological forces that make doing the right thing so difficult in the first place.
What Happens When Lifestyle Is Combined With GLP-1 Therapy?
This is where the argument becomes testable. If obesity was primarily a matter of knowing what to do, then lifestyle counseling alone should perform nearly as well as lifestyle counseling plus medication. After all, both groups receive the advice. Both groups are told to reduce calories. Both groups are encouraged to increase physical activity. Both groups are followed in a clinical trial.
That is not what happens.
The GLP-1 and GIP/GLP-1 trials did not compare medication against nothing. They compared medication plus lifestyle intervention against placebo plus lifestyle intervention. That distinction matters. The placebo group was not abandoned in the parking lot, with a pamphlet and a pat on the back. They received structured lifestyle guidance inside a randomized clinical trial, with calorie goals, activity goals, behavioral counseling, and scheduled follow-up.
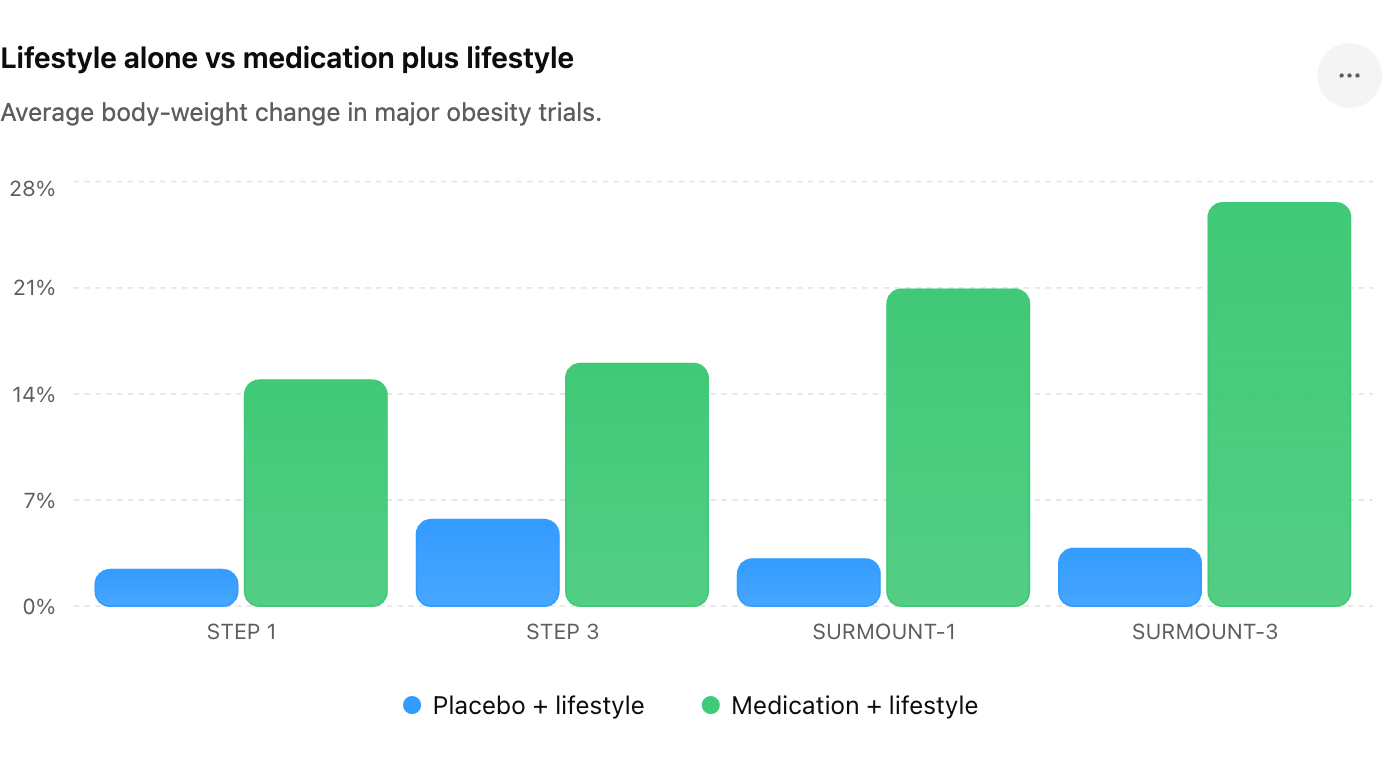
In STEP 1, participants received lifestyle intervention and were randomized to semaglutide 2.4 mg or placebo for 68 weeks. The semaglutide group lost about 14.9% of body weight. The placebo group, receiving the same lifestyle foundation without active drug, lost about 2.4%. That is not a small difference. That is the difference between lifestyle advice acting alone and lifestyle advice paired with a medication that changes hunger and satiety biology.
STEP 3 made the lifestyle component even more rigorous. Participants received intensive behavioral therapy, including frequent counseling visits, calorie targets, physical activity goals, and an initial low-calorie diet. If the criticism is that lifestyle arms are too weak, STEP 3 is the answer. The placebo plus intensive behavioral therapy group lost 5.7% of body weight. The semaglutide plus intensive behavioral therapy group lost 16.0%.
Then came tirzepatide.
In SURMOUNT-1, participants receiving tirzepatide lost up to about 20.9% of body weight at 72 weeks, while the placebo plus lifestyle group lost about 3.1%. Again, both groups received lifestyle intervention. The difference was not that one group discovered vegetables, protein, walking, or calorie awareness. The difference was the medication.
SURMOUNT-3 is perhaps the most useful study for this discussion, because it began with intensive lifestyle intervention before randomization. Participants first completed a 12-week lifestyle lead-in. This was not casual advice. They received frequent counseling, calorie targets of about 1,200 calories per day for women and 1,500 calories per day for men, up to two meal replacements per day, a goal of at least 150 minutes per week of moderate physical activity, behavior modification strategies, and food and exercise logs. Only those who lost at least 5% of their body weight during that lead-in period were randomized.
In other words, SURMOUNT-3 selected people who had already demonstrated they could respond to lifestyle intervention. These were not people unwilling to do the work. They had already done it.
Then the study asked the real question: after successful lifestyle-induced weight loss, what happens next?
Those randomized to tirzepatide lost substantially more weight. Those randomized to placebo, despite having already succeeded with lifestyle intervention, did not continue on the same trajectory. The medication group reached an average weight loss of about 26.6% from the start of the lifestyle lead-in, compared with about 3.8% in the placebo group.
That is the thermostat analogy in trial form. Lifestyle opened the window. The body began to push back. Tirzepatide changed the system enough that the weight continued to fall, rather than drift back toward the old setting.
This is why the phrase “GLP-1 just helps people do the right thing” is incomplete. Yes, people eat less on these medications. Yes, they often make better food decisions. Yes, lifestyle still matters. But the reason they can sustain those behaviors is that the biological pressure has changed.
The placebo arms already tested the lifestyle-only argument. They received the advice. They received the counseling. In some trials, they received intensive behavioral therapy. In SURMOUNT-3, they had already lost weight before randomization.
The drug was still the difference.
That does not make lifestyle irrelevant. It makes lifestyle more achievable. Exercise still protects muscle, improves insulin sensitivity, improves cardiorespiratory fitness, and helps long-term maintenance. Nutrition still matters, because weight loss alone is not the same as health. Protein, fiber, fruits, vegetables, legumes, whole grains, and healthy fats still matter.
But the evidence is clear: for most patients, lifestyle intervention alone produces modest average weight loss, while lifestyle plus GLP-1 or GIP/GLP-1 therapy produces substantially greater weight loss. That is not because people suddenly learned what to do. It is because biology finally stopped fighting them with the same intensity.
Conclusion: GLP-1 Gives Us a Fair Shot
The lesson of the GLP-1 era is not that lifestyle is insignificant. If anything, the opposite is true. It is an important part, but it cannot be the only part - at least for the majority of us.
Exercise still improves fitness, preserves muscle, improves insulin sensitivity, and contributes to long-term health. Good nutrition still matters. Fruits, vegetables, legumes, whole grains, healthy fats, and adequate protein remain the foundation of health whether someone takes a medication or not.
The lesson is that obesity was never simply a knowledge problem.
We know what successful people do. We have known for decades. We know how to lose weight. We know how to exercise. We know how to improve nutrition. We know how to track calories. We know how to create a calorie deficit.
What we have struggled with is helping people sustain those behaviors, while their biology actively pushes them in the opposite direction.
The placebo arms of the modern obesity trials answered an important question. Lifestyle intervention works. It produces meaningful health benefits and modest weight loss. But when medications that alter hunger, satiety, and food reward are added, weight loss becomes substantially greater and more durable.
That does not mean GLP-1 medications are magic.
It means they give millions of people something they have rarely had before: a fair fight.
For decades, obesity treatment asked patients to overpower biology through willpower alone. Many succeeded temporarily. Some succeeded long term. Most struggled.
GLP-1 therapy does not replace healthy habits. It makes those habits easier to sustain.
And for many people, that difference changes everything. And I am one of those people.
