

News of the Week in Medicine
Ebola, Hantavirus, Telemedicine, Pancreatic Cancer, Ice Cream Recalls, and Why Public Health Only Looks Invisible When It Works

This week in medicine felt like a collision between two futures.
One future is hopeful: precision cancer drugs once thought impossible are extending lives. Telemedicine continues to reshape healthcare delivery, and even simple habits like walking are more powerful than wellness influencers often admit.
The other future is darker: Ebola spreading through central Africa without an approved vaccine for the circulating strain, hantavirus clusters triggering international monitoring efforts, and public-health systems weakened after years of political exhaustion and distrust.
Medicine always lives in this tension.
Scientific progress moves forward while public confidence lurches backward.
And increasingly, the systems that quietly protect modern civilization are only noticed when they begin to fail.
WHO Declares Ebola a Global Health Emergency
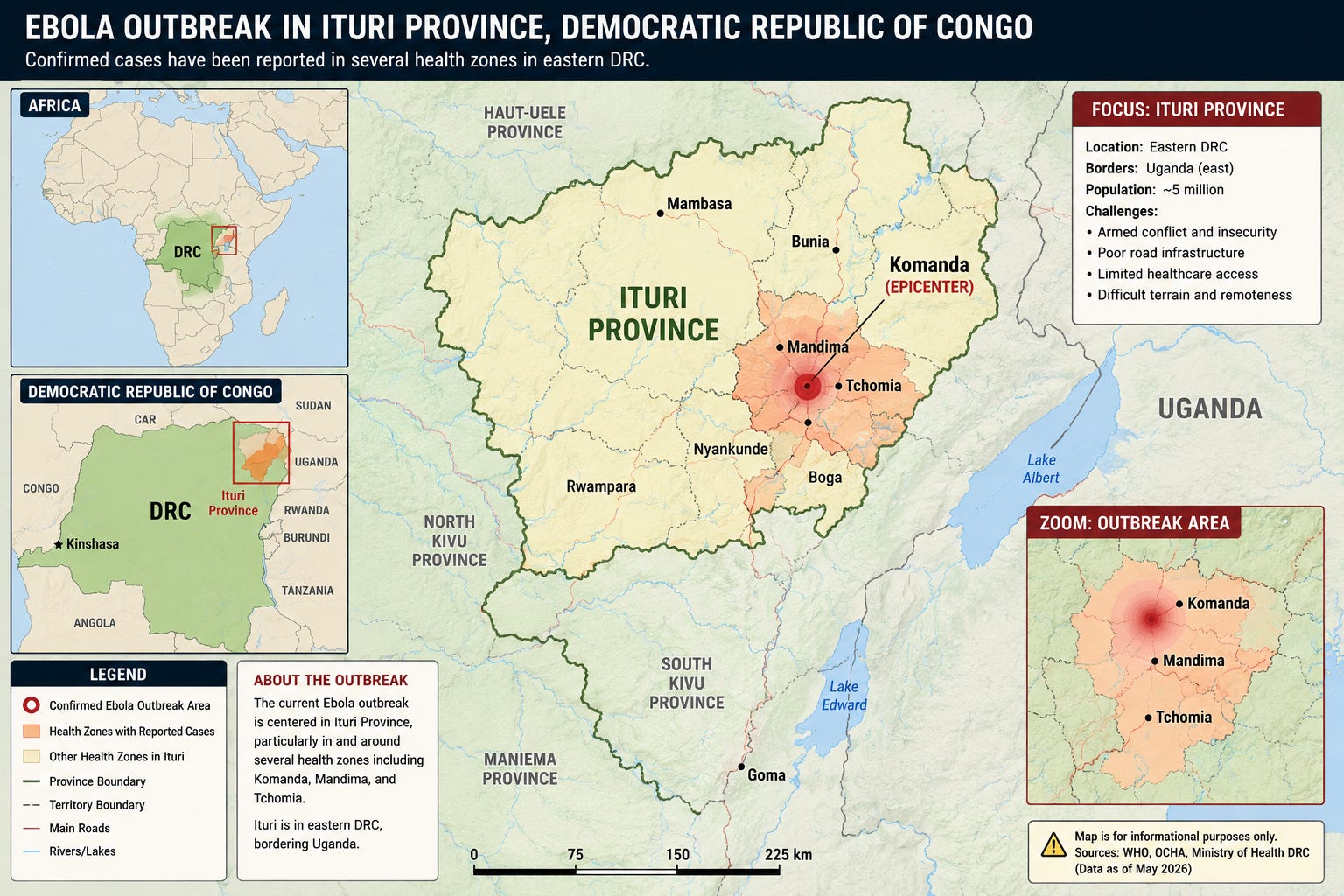
The World Health Organization officially declared the Ebola outbreak spreading through the Democratic Republic of Congo and Uganda a “Public Health Emergency of International Concern” — the organization’s highest warning level short of declaring a pandemic.
That phrase sounds bureaucratic. It is not.
It means the world’s leading infectious disease experts believe this outbreak poses enough international risk to require coordinated global action before it spreads further.
And there are reasons for concern.
This outbreak appears to involve the Bundibugyo strain of Ebola, rather than the classic Zaire strain responsible for previous outbreaks.
That matters enormously, because the currently licensed Ebola vaccines were designed against the Zaire strain.
At this moment, there is no approved vaccine specifically for Bundibugyo Ebola.
The outbreak is also occurring in one of the most difficult environments imaginable for infectious disease control: eastern Congo, a region fragmented by militia violence, poor infrastructure, displaced populations, weak healthcare systems, and ongoing humanitarian instability.
Getting supplies into these regions is extraordinarily difficult.
Protective equipment travels through conflict zones. Refrigeration chains fail. Roads disappear in heavy rains. Laboratory samples may take days to move safely. Communication between rural clinics and national authorities can collapse entirely.
And a heroic doctor does not stop outbreaks holding a syringe.
They are stopped by logistics.
Fuel. Gloves. IV fluids. Refrigeration. Mobile labs. Contact tracers. Burial teams. Secure transport routes. Community trust.
Containment is infrastructure.
During the 2014–2016 West African Ebola epidemic, the United States and WHO aggressively intervened. CDC teams entered outbreak zones. Mobile laboratories were built. Field hospitals were established. Teams were deployed to safely handle and bury the dead, because Ebola remains highly contagious after death.
I remember this personally.
At the time, I was chairman of surgery, and we held meetings preparing for Ebola’s possible arrival in the United States. Isolation rooms were designated. PPE stockpiles were checked. Protocols were rehearsed. We were told to expect Ebola.
The reason widespread transmission never happened here was not luck.
It was intervention.
We helped contain the outbreak there before it became catastrophic here.
That infrastructure is weaker now.
The United States withdrew from WHO and cut funding to the organization that historically coordinated international outbreak response. CDC staffing has also been substantially reduced. The institutions that once served as the backbone of epidemic response are now politically controversial.
Viruses do not care.
This is where many Americans first learned about Dr. Craig Spencer, the New York physician who survived Ebola after treating patients in West Africa. He recently discussed the emotional and physical reality healthcare workers face when confronting dangerous pathogens firsthand and why preparation matters before panic begins.
One of the recurring themes of infectious disease is that humans consistently misunderstand risk.
We fear cinematic catastrophes while ignoring ecological realities.
Hantavirus is fundamentally an ecological disease. Rodent populations expand after favorable climate conditions. Humans encounter contaminated droppings in cabins, garages, sheds, campsites, barns, and poorly ventilated spaces. Exposure happens quietly and accidentally.
And once again, prevention comes down to boring but essential infrastructure:
surveillance,
laboratory capacity,
environmental monitoring,
communication systems,
rapid testing,
and coordinated public-health response.
The same systems that detect Ebola in central Africa help identify unusual respiratory clusters in Colorado, Nebraska, or Illinois.
Public health is interconnected.
Hantavirus and the Ecology Problem
Public health officials are also continuing to monitor the multinational hantavirus cluster linked to the MV Hondius cruise ship outbreak.
The latest CDC updates emphasize that there are currently no confirmed U.S. cases of the Andes hantavirus strain responsible for the outbreak, and public risk remains very low. (CDC)
Still, dozens of Americans are being monitored after exposure during the cruise outbreak. (American Hospital Association)
The Andes strain matters because unlike the North American Sin Nombre strain typically seen in the United States, Andes hantavirus can occasionally spread person-to-person through prolonged close exposure. (Reuters)
The Supreme Court and the Quiet Telemedicine Revolution
This week, the Supreme Court also allowed continued access to mifepristone by mail, while litigation continues in lower courts.
That may sound like a narrow abortion story.
It is also a telemedicine story.
COVID permanently accelerated one of the largest shifts in healthcare delivery in modern history: medicine partially leaving buildings and entering digital space.
Patients now routinely receive care remotely. Prescriptions arrive by mail. Mental-health visits happen virtually. Chronic diseases are managed online. Geographic barriers matter less than they once did.
And regardless of political views about abortion, this case highlights a deeper unresolved question:
What happens when healthcare no longer respects state borders the way old medical systems assumed it would?
Technology has already changed medicine.
The legal system is still catching up.
A Pancreatic Cancer Breakthrough Once Thought Impossible
And amid all the anxiety this week, there was also extraordinary news from cancer research.
An experimental drug called daraxonrasib significantly prolonged survival in patients with advanced pancreatic cancer.
That is an astonishing sentence in oncology.
Pancreatic cancer has long been one of the most lethal and discouraging diagnoses in medicine. For decades, scientists unsuccessfully targeted a protein called KRAS, which drives many pancreatic, colon, and lung cancers.
Researchers referred to KRAS as “undruggable.”
And then science did what science occasionally does best: it proved its own assumptions wrong.
After decades of failures, publicly funded NIH research, academic laboratories, and biotech companies slowly identified vulnerabilities in KRAS that eventually allowed a drug to disable it.
Patients receiving daraxonrasib survived a median of more than 13 months, compared with less than seven months for chemotherapy patients.
That is not a cure.
But in pancreatic cancer, it is enormous progress.
And it is also a reminder that scientific progress often looks inefficient right up until the moment it changes lives.
Ice Cream, Metal Fragments, and Why Food Safety Matters
Meanwhile, Straus Family Creamery voluntarily recalled several organic ice cream flavors after concerns about possible metal contamination in certain production batches.
No injuries were reported.
Which is exactly the point.
Modern food safety systems work because they identify problems before many people are harmed. The FDA, epidemiologists, manufacturing oversight, traceability systems, and recall infrastructure are all part of the same invisible public-health architecture most people never notice.
Milk used to routinely kill people.
Foodborne outbreaks once devastated communities.
Now we complain when a company voluntarily recalls ice cream before anyone gets hurt. Yes, I love ice cream–if only my intestines had more lactase.
That annoyance is actually evidence of success.
Maybe Walking Still Works Better Than Biohacking
And finally, one of my favorite studies of the week.
Researchers found that people averaging roughly 8,500 steps daily during weight-loss programs were significantly more successful at maintaining weight loss long term.
Not 30,000 steps.
Not cold plunges.
Not wearable optimization systems.
Walking.
There is something wonderfully humbling about that.
Modern wellness culture often swings between extremes: either obsessive optimization or complete resignation. But most durable health improvements still emerge from remarkably ordinary behaviors repeated consistently:
walking,
sleeping,
resistance training,
social connection,
eating fewer ultra-processed foods,
spending time outside.
The body still responds beautifully to consistency.
And increasingly, obesity medicine and GLP-1 science are reinforcing something many physicians quietly suspected for years:
The best intervention is often the one people can actually continue doing. You can measure your steps with almost any device, but once you have the route you will travel, just keep doing it. This is about 4 miles of walking.
The Larger Story
The larger story this week is not merely Ebola, hantavirus, cancer drugs, abortion pills, food recalls, or walking studies.
It is the strange contradiction of modern medicine itself.
We are simultaneously:
more scientifically capable than ever,
and more socially distrustful than ever.
We are sequencing viruses faster while questioning epidemiology.
We are developing molecular cancer therapies while dismantling pieces of public-health infrastructure.
We expect miracles from medicine while growing suspicious of the institutions that produce them.
And yet medicine keeps moving forward anyway.
Sometimes awkwardly.
Sometimes politically.
Sometimes inefficiently.
But forward nonetheless.
The danger is not simply that dangerous viruses exist.
The danger is that societies begin mistaking the absence of catastrophe for proof the systems preventing catastrophe were unnecessary all along.
