

Particles to Plaque — Part Two
From Silent Disease to Heart Attack

Why the “lipid hypothesis” is no longer a hypothesis
You will still hear people talk about “the lipid hypothesis of heart disease.”
At this point, that phrase is mostly a relic.
In the 1950s, cholesterol’s role in heart disease was inferred from population data and early experiments. Calling it a hypothesis made sense then.
It does not now. When carnivores talk about the hypothesis they are going back 70 years, we know how lipids work, as we said in the previous work.
Today we have a mechanism. We have human genetics. We have pathology, molecular biology, and outcomes data that all tell the same story. Atherosclerotic heart disease is no longer an idea waiting for confirmation. It is a process we can trace — from circulating particles, to plaque formation, to rupture, to clot, to heart attack.
In the previous chapter, we walked through how ApoB-containing particles enter the arterial wall and form plaques. Now we move to what happens after those plaques exist.
Because heart attacks are not sudden accidents.
They are the final event in a long, quiet disease.
When you can see the danger in time
Let me start with a story.
My father-in-law, George, was living in China and preparing for a routine colonoscopy. Because he had previously had a coronary stent placed, his doctors decided — almost as an aside — to do a CT scan of his heart.
That scan changed everything.
It showed a 90 percent obstructing lesion in the left main coronary artery — the point where two of the three major coronary arteries arise. Cardiologists call this area the widowmaker for a reason. If a plaque ruptures, in that part of the artery, it will then cause a sudden clot, and death is often immediate.
George’s doctor advised him to address it when he returned to the United States, and sent me the images before he arrived. When I saw them, I arranged for him to see my favorite cardiologist at Arizona Heart Hospital the day after he arrived.
When George arrived with his images, the cardiologist didn’t talk about scheduling.
He admitted him directly to the hospital.
That afternoon, George had a new stent placed.
To the cardiologist, that plaque looked like a keg of dynamite with a short fuse. It wasn’t causing pain yet. It wasn’t fully blocking blood flow. But if it ruptured, there would be no second chance.
George is alive because someone saw the plaque before it declared itself.
That plaque did not appear overnight. It formed slowly, silently, over years — exactly the process we discussed in Part One.
Most people don’t get that warning.
How heart disease usually reveals itself
Here is the uncomfortable truth.
About 25 percent of people with coronary artery disease are first diagnosed at death. Sudden cardiac death is not rare. It is a common first presentation.
For many others, the first sign of heart disease is a heart attack.
Not months of warning symptoms.
Not a gradual decline.
But a sudden, life-altering event.
This happens because atherosclerosis hides well.
Plaques grow quietly. Arteries remodel outward. Blood flow stays normal. Stress tests are negative. EKGs look fine. People feel well.
Detection lags behind biology.
This is why so much heart disease is discovered after a heart attack rather than before it.
Why plaque size doesn’t predict heart attacks
For decades, heart disease was imagined as a plumbing problem — arteries slowly narrowing until blood could no longer get through.
That model is wrong.
Most heart attacks occur in arteries that were not severely narrowed beforehand.
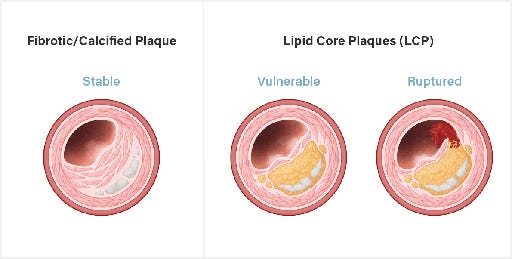
The most dangerous plaques are often:
relatively small
not very obstructive
rich in lipid
covered by thin, fragile fibrous caps
These plaques may never cause angina. They may not limit flow. They may not show up on stress testing.
Yet they are the plaques most likely to rupture.
Large, heavily calcified plaques may narrow arteries but often remain stable for years. Statins tend to stabilize the plaque, causing calcification and increasing the cap of the plaque to decrease the risk of plaque rupture.
Size does not determine danger. Structure does.
From rupture to catastrophe
When the surface of a plaque ruptures, everything changes — fast.
The contents of the plaque are suddenly exposed to the bloodstream. The body interprets this as injury.
Platelets activate.
A clot forms.
Blood flow drops or stops.
If the artery is completely blocked, the result may be sudden cardiac death. If partially blocked, the result is a heart attack with permanent damage.
Where the rupture occurs matters enormously. A rupture in a small branch may be survivable. A rupture in a major artery — especially near the origin of the coronary circulation — can be immediately fatal.
Same disease.
Same biology.
Different outcome.
When there is no warning at all
Now let me tell you another story.
My brother, Jimmy.
One day, he felt crushing chest pain. He knew exactly what it was. He dialed 911.
His wife told him she could get him to the hospital faster. He waved her off. (We are stubborn Simpsons.)
The ambulance arrived and loaded him in.
On the way to the hospital, my brother’s heart stopped three times.
Three times.
And three times, the paramedics shocked him back with electricity.
Had he driven himself, he would have died.
Had his wife driven him, he would have died.
Because he was in an ambulance — with monitors, medications, and defibrillators — he lived.
Jimmy went on to have open-heart surgery. He quit smoking. He started taking statins. He changed his life.
Jimmy has the same disease I have.
The difference was not toughness. It was not willpower.
It was making the right call at the right moment.
Why you call 911 — and don’t “grunt it out”
Heart attacks are not just about blocked arteries. They are also about lethal heart rhythms.
Ventricular fibrillation can occur without warning. When it does, seconds matter. Paramedics can treat it immediately. Cars cannot.
Ambulances also:
start treatment right away
transmit EKGs before arrival
take you directly to a cardiac-capable hospital
Driving yourself — or being driven — removes your safety net.
Many people who die from heart attacks never reach the hospital.
Jimmy is alive because he didn’t try to tough it out.
The quiet truth
Atherosclerosis is years in the making.
Heart attacks happen in minutes.
By the time pain begins, the disease has already made its move. The only question left is how fast help arrives.
This is why prevention matters.
This is why early detection matters.
And this is why, when symptoms appear, you don’t negotiate with them.
You call 911.
Selected references (free section)
Coronary Atherosclerosis: Determinants of Plaque Rupture.European Heart Journal. 1998. Grønholdt ML, Dalager-Pedersen S, Falk E.
2 Mechanisms of Acute Coronary Syndromes and Their Implications for Therapy.The New England Journal of Medicine. 2013. Libby P.
3.Why Do Plaques Rupture?.Circulation. 1992. Falk E.
4.Relationship Between Calcified Plaque Burden, Vascular Inflammation, and Plaque Vulnerability in Patients With Coronary Atherosclerosis.JACC. Cardiovascular Imaging. 2024. Fujimoto D, Kinoshita D, Suzuki K, et al.
5 Calcification in Atherosclerotic Plaque Vulnerability: Friend or Foe?.Frontiers in Physiology. 2020. Shi X, Gao J, Lv Q, et al.
6.Relationship Between Coronary Artery Calcification and Plaque Vulnerability, a Qualitative and Quantitative Optical Coherence Tomography Study.International Journal of Cardiology. 2025. Liu C, Yang F, Hu Y, et al.New
7.Calcium Deposition Within Coronary Atherosclerotic Lesion: Implications for Plaque Stability.Atherosclerosis. 2020. Jinnouchi H, Sato Y, Sakamoto A, et al
Paid Section — What Happens After the Plaque Ruptures
By the time a plaque ruptures, the disease has already done its work.
What follows next determines how much heart muscle is lost, whether a person survives, and what kind of life they have afterwards.To understand that, we need to be precise about what happens in the minutes to hours after the rupture.
