

The Cancer Spike That Wasn’t — And Why the Vaccine Got Blamed Anyway
When raw numbers go viral and context quietly exits the room

The anti-vaccine crowd claims “victory”, blaming the COVID vax for a rise in cancers.
A new set of cancer numbers dropped, and for about a day and a half the internet did what it does best — found a number, stripped it of context, and declared the case closed.
Cancers in people under 50 were “up 6.4%.” Must be the turbo-cancer of the vaccines.
That was enough. No pause. No curiosity. Just a straight line drawn from that number to the conclusion: vaccines.
And then, just as quickly, the story faded. Not because the data disappeared — but because once you actually look at it, the conclusion doesn’t hold up.

Because here’s the part that never makes it into the viral posts: some of these cancers have been rising for decades.
Early-onset colorectal cancer didn’t begin in 2021. It didn’t begin in 2020. The curve starts bending upward long before COVID, long before mRNA vaccines, long before any of the current talking points. In fact, it started rising in the mid 1980’s.
So if the explanation you’re offering requires a starting point in 2021, but the data clearly start in the 1980s, that’s not a bold hypothesis, or some new discovery. That is inconvienient data that is best ignored.
COVID and lack of Cancer Screening
Then there’s the pandemic itself — another variable that gets conveniently skipped. Remember during the pre-vaccine times in the pandemic, when you couldn’t go to the hospital because it was overwhelmed?
During COVID, cancer screenings dropped. Colonoscopies were delayed. People stayed home. Health systems were strained. When that happens, diagnoses don’t disappear — they get pushed forward.
So when normal care resumes, you see a rebound. Not because cancer suddenly appeared, not because cancer burst out from vaccines, but because it’s being found after a delay. The mammogram that wasn’t done because they were sheltering in place, or the colonoscopy cancelled, and now we find a tumor.
What We’ve Actually Won — And It Matters
It’s easy to miss this part because it doesn’t trend, but it should.
We are better at preventing and treating cancer than we’ve ever been.
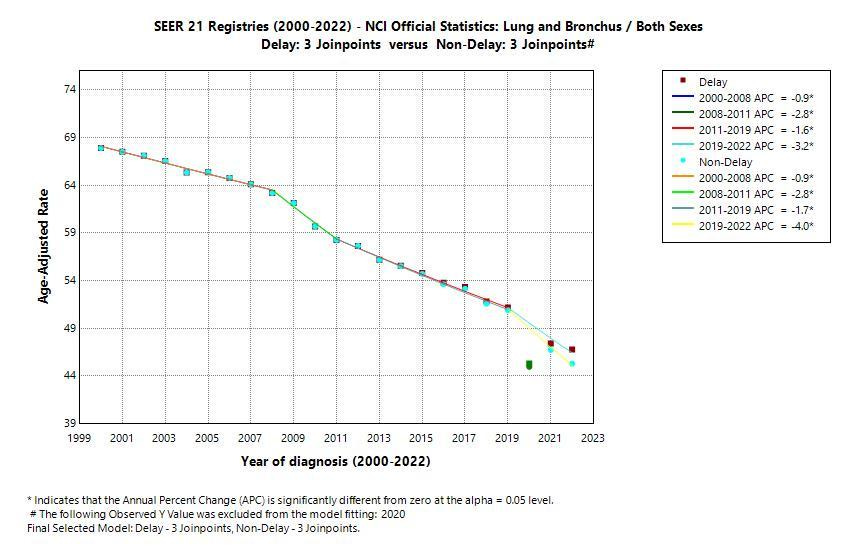
Lung cancer deaths have fallen — not because of a miracle drug, but because fewer people smoke. That’s public health working exactly as intended.
Cervical cancer has dropped dramatically in screened populations and continues to fall with HPV vaccination. That’s prevention layered on top of early detection.
Colon cancer deaths in older adults have declined, largely because we find and remove precancerous polyps before they ever become cancer. That’s not treatment — that’s interruption of the disease itself.
And across multiple cancers, survival has improved with better surgery, targeted therapies, and immunotherapy. Not perfect. Not evenly distributed. But real progress.
So when someone tells you “nothing is working,” they ignore decades of measurable, repeatable gains.
Early Detection — Why the Numbers Can Look Worse Before They Look Better
Screening complicates the story, and that’s where many people get lost.
When you look harder, you find more. This is the story of breast cancer. When I was a surgical resident, we found breast cancers by examinations. As technology of mammography improved, we started finding smaller breast cancers with mammograms. Smaller cancers, earlier detection, earlier treatment, and we went from 75% five year survival to 99% five year survival and cures.
That means:
More early-stage cancers were detected
More “cases” counted
Sometimes a temporary rise in incidence
But catching cancer earlier is exactly what reduces death.
A colonoscopy doesn’t just detect cancer — it prevents it. A mammogram finds tumors before they spread. HPV testing identifies risk before cancer develops.
So yes, better detection can make the numbers look worse on the surface. But underneath, it’s shifting cancers into stages where we can actually do something about them.
If you only look at case counts without understanding detection, you can convince yourself that things are getting worse when, in fact, outcomes are improving.
Cancer deaths, by the way, with one glaring exception, are going down.
Smoking, Public Health, and What Actually Works
If you want a clean example of medicine and public health getting it right, look at smoking.
In the mid-20th century, smoking was everywhere — culturally accepted, heavily advertised, even wrapped in a kind of manufactured credibility. You’ll still see people drag out those old Camel ads with physicians in white coats, as if that somehow indicts modern medicine. It doesn’t. It shows how marketing worked.
What changed wasn’t a grassroots epiphany or sudden shift in personal responsibility. It was leadership. It was data. And it was institutions willing to act on both.
The turning point came with the 1964 Surgeon General’s Report on Smoking and Health — a moment when the evidence became impossible to ignore, and the federal government said so clearly and publicly. From there came warning labels, advertising restrictions, public campaigns, and eventually indoor smoking bans.
And here’s the part that gets conveniently left out: no major medical organization endorsed smoking once the evidence was clear. Quite the opposite. The entire weight of public health moved in one direction.
The result? Smoking rates fell. And with them, lung cancer deaths began to decline. Not overnight, not perfectly, but steadily and measurably.
That’s what success looks like in medicine — not perfection, but progress that shows up in real populations over time.
There’s still work to do. Smoking hasn’t disappeared, and lung cancer hasn’t either. But the next frontier isn’t pretending cigarettes were harmless — it’s recognizing that air quality matters more than ever.
Wildfire smoke, urban pollution, fine particulate matter — these are not trivial exposures. They increase the risk of lung cancer, even in people who have never smoked, and likely contribute to other cancers.
So the lesson isn’t that public health got it wrong.
The lesson is that when we identify a real risk, measure it carefully, and act on it consistently — we reduce disease.
What Is Rising — And Why We’re Paying Attention
Now here’s the part that deserves concern.
Some cancers, particularly in younger adults, are rising. Early-onset colorectal cancer is the one that has everyone’s attention, and it should.
But again, this didn’t start in 2021. It started in the 1980’s, and perhaps even earlier.
This has been building for decades, and the likely drivers are not mysterious:
Increasing obesity
Changes in diet, especially ultra-processed foods
Microbiome alterations
Sedentary behavior
Metabolic dysfunction
None of these flipped on overnight. None of them align with a single event.
This is what a real public health problem looks like — gradual, multifactorial, and frustratingly resistant to simple answers.
Which is exactly why it gets replaced online with a simple answer. Cancers don’t happen overnight, they happen when they are in an environment that leads to progressive damage to a person’s DNA.
This is why we are now focusing on cancers due to the other lifestyles - food, metabolic disorders, and obesity. This will be the GLP-1 shift, as obesity drops, so will these cancers. As fiber is incorporated into the diet, so will these tumors decrease.
Turbo Cancer
And then there is this term. Turbo cancer. It is not a real term. But sometimes it seems like cancer goes fast.
Find a cancer that is widespread, which we do all too often, and it kills quickly. This is nothing new, this is cancer. This is why we focus on early detection, because if we detect early, we prevent a cancer from widespread metastasis.
Still, the anti-vax crowd took this term and is running with it. And every person with a friend or relative with widespread cancer adopts it. It isn’t from the vaccine, it is the nature of cancer.
Vaccines are Easy to Blame
Blaming vaccines works because it’s simple. One cause. One villain. No need to wrestle with decades of shifting diet patterns, metabolic disease, or screening behavior.
The one “cause” is the mark of a huckster. Today it is vaccines, yesterday it was a parasite, who knows what one thing it will be tomorrow.
Complex problems are frustrating. Simple answers are comforting.
Even when they’re wrong. And there is an industry based on cancer caused by the COVID vaccines. Charlatans are already selling detoxification (there is no such thing). It is in an enema form, god knows why these people love their enemas. From coffee to god knows what.
And if there were a real signal — something meaningful, something large enough to move population-level cancer rates — it wouldn’t show up as a selective, inconsistent pattern that appears in one age group, one time window, and nowhere else.
It would be obvious. It would be reproducible. It would be everywhere.
That’s how epidemiology works. Signals don’t whisper.
So what happened to the story?
Nothing mysterious. It just didn’t survive contact with the full dataset.
The headline traveled. The correction didn’t.
Closing
What we’re watching isn’t the emergence of a new truth. It’s the recycling of an old habit — start with a conclusion, find a number that sounds alarming, and ignore everything that complicates it.
The data didn’t go anywhere. They’re still there, doing what data do — quietly resisting oversimplification.