

The Diabetes Mystery
The Clue That Changed How We Think About Diabetes

Why the story of diabetes changed—and why that matters
One of my favorite sayings is that in science, we love to be proven wrong.
Not because we enjoy being embarrassed. Not because we enjoy discovering that years of teaching, research, and clinical experience were incomplete. We love being proven wrong, because whenever nature proves us wrong, she usually has a more elegant solution than the one we started with.
The story of type 2 diabetes is one of those moments. Probably what you think about adult onset diabetes is from our old model. A model that served us well, and still does.
This is not one of those articles that begins with, “Everything you’ve been told is a lie.” Usually when somebody says that, they are about to sell you a supplement, a diet book, or a conspiracy theory.
Instead, this is the story of how medicine changed its understanding of a disease that affects millions of Americans. It is a story of clinical observations, laboratory discoveries, arguments between scientists, and a handful of stubborn facts that refused to fit the model we were using.
Because if you understand how type 2 diabetes actually develops, you won’t be fooled when somebody tells you they can cure it. You’ll understand why bariatric surgery can place diabetes into remission. You’ll understand why GLP-1 medications work so well. You’ll understand why fasting sometimes works, why weight regain can bring diabetes back, and why the word “remission” is usually more accurate than the word “cure.”
Most importantly, you’ll understand why sugar is probably not the villain most people think.
Sugar is more like the person standing over the body holding the knife when the detective walks into the room.
It certainly looks guilty. And blood sugar is involved. But it isn’t the whole story.
For most of my career, the explanation for type 2 diabetes seemed straightforward. People gained weight, became insulin resistant, their pancreas worked harder and harder until eventually it could not keep up. Blood sugars rose. Medications were added. More medications were added. Eventually insulin entered the picture. Lose enough weight and diabetes improved, because insulin resistance improved.
Simple. Elegant. Mostly right.
One of the reasons we performed bariatric surgery on patients with obesity and type 2 diabetes was because we expected exactly that sequence of events. Weight comes down. Diabetes gets better. Lose enough weight and medications can be reduced. Lose more weight, and perhaps the patient no longer needs them.
Even insurance companies eventually accepted that logic. And if you’ve ever worked with insurance companies, getting them to agree to pay for something is roughly equivalent to convincing a Venetian gondolier to install a freeway.
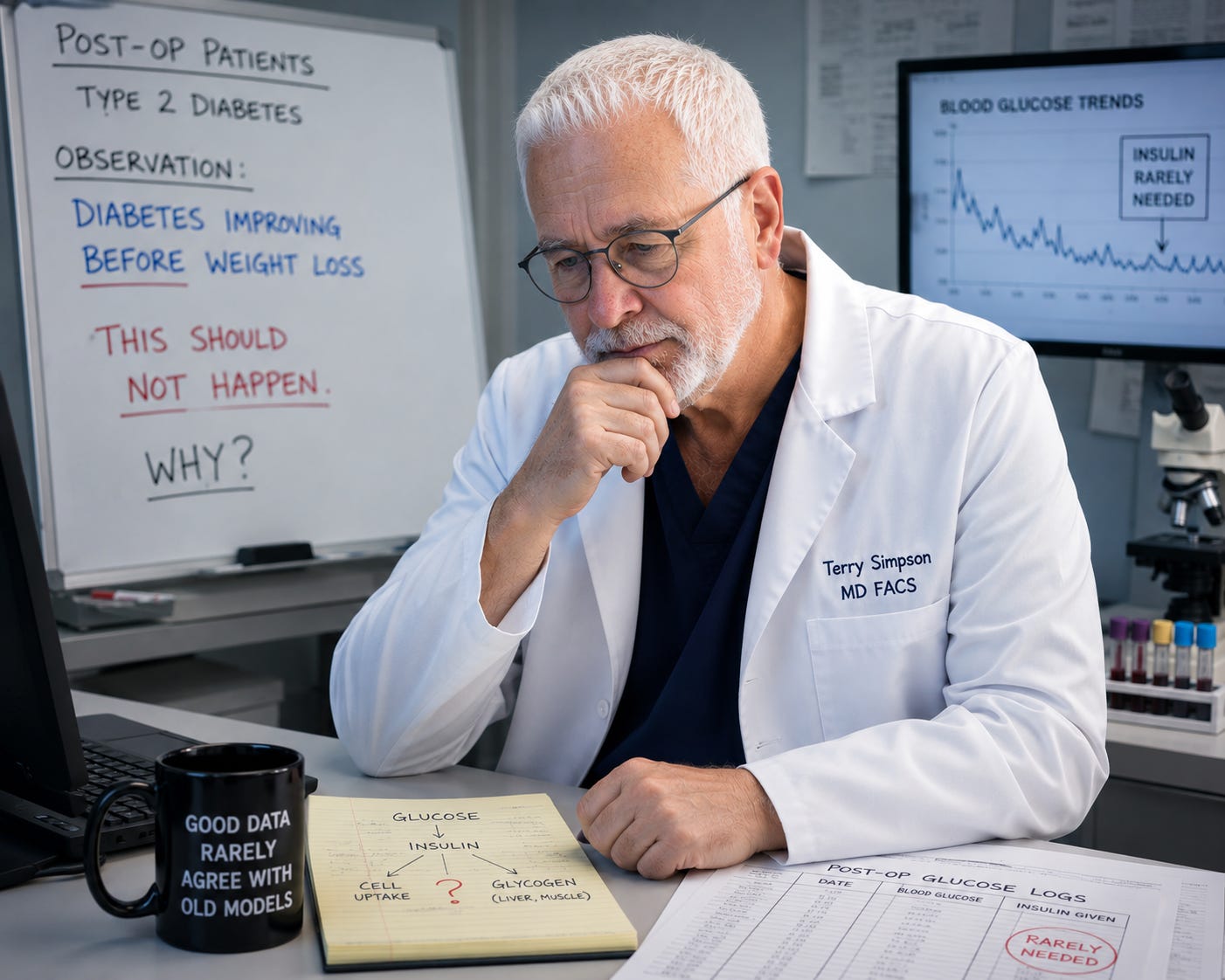
Here comes the mystery, though. My weight loss surgery patients did not follow that model’s timeline. Diabetes was improving before weight loss, and that should not have happened. The entire logic of the model predicted the opposite sequence. Weight loss first. Better diabetic control second. Instead, the body seemed determined to rearrange the order of events.
The Observation
Like most surgeons, I operated on patients with obesity and type 2 diabetes. Some were taking insulin. Some were taking enough insulin that forgetting it on vacation caused more panic than forgetting their wallet. Others were on metformin, a sulfonylurea, and whatever new diabetes medication the pharmaceutical industry had recently named after what sounded like a Scandinavian airport.
But let me separate the weight loss surgery patients from the other patients. In these cases, the operation would go well. They would spend a night or two in the hospital. Like every surgeon, I left orders for blood sugar checks and insulin coverage if needed. Pretty standard stuff.
The moment I realized something strange was happening came early in my career.
I got a call from the emergency room about one of my postoperative patients. She had surgery a few days earlier, went home, followed her instructions, took her diabetes medications exactly as prescribed, and ended up in the ER with dangerously low blood sugar.
At first I thought it was an isolated event. One patient, one strange reaction, one of those things medicine files away under “well, that was interesting.”
Then it happened to another patient.
That is when I stopped automatically telling patients to resume their diabetes medications after surgery. Instead, I told them to watch their blood sugars and only restart medication if the numbers began climbing.
In the hospital, we never order their usual medicines for diabetes. Patients are without food, so they might not be eating enough, or not at all, so we would inadvertently drive their glucose too low. Or events can happen that drive sugar up. So most of the time, we write a sliding scale for our surgical patients, so nurses check the blood glucose and add insulin based on their glucose level. Sometimes our scale is too conservative, and we get a call from the nurses that the blood sugars are high and we need to add more short acting insulin. Rarely the opposite happens. In the hospital, our preference is to go up rather than down. So our scale starts with a small amount of insulin to cover higher blood sugars.
After those two patients had low blood sugars, I noticed that my weight loss surgery patients did not generate calls from the nurses about insulin. That was not the case with patients who had other operations - like colon surgery, or removing a gallbladder. Non weight loss patients with obesity and diabetes, I received calls to adjust the insulin.
Surgeons notice patterns. We especially notice patterns at two o'clock in the morning. Before long, I realized I was sleeping through nights for weight loss surgery patients.
The Review
That seemed like more than a coincidence. So I went back and looked at the data. I reviewed the hospital glucose logs for my surgical patients. I looked at the sliding-scale insulin orders I had dutifully written after surgery.
The funny thing was that the insulin was rarely given for weight loss surgery patients. The orders were there. The insulin was available. The blood sugars were all pretty normal, and the patients didn’t need the short-acting insulin.
The exception was the first 24 hours, as the operation itself raises blood sugar. Surgery is a stress to the body, and cortisol goes up. Stress hormones rise. The body reacts to being operated on in much the same way most people react to seeing their first hospital bill. There is a stress response.
What didn’t make sense was how many patients never needed coverage at all. Then they would return to the clinic. I assumed they would be a bit on the “sweet” side, with higher blood sugars, and need to have medicine restarted. But they didn’t.
Weeks later, many still weren’t taking insulin or metformin. Months later, some still weren’t.
Why Did Diabetes Improve Before Weight Loss
Diabetes improved before weight loss. That didn’t fit the conventional model. Somehow the body had gotten the message before the scale did. The pancreas produced enough insulin, and the cells were sensitive to that insulin long before enough weight had disappeared to explain it.
It is not that my surgical stapler replaced an endocrine organ, although we now call ourselves “Metabolic and Bariatric Surgeons.” It is because the body indeed had a far more interesting role, and diabetes is more interesting than we knew.
In science, we build models to explain nature. Dogma never wants to be wrong. But in science, we love when we are proven wrong. Because that means mother nature has a more elegant solution.
The Hormone That Changed Medicine
To understand why the pancreas got the message before the scale did, we need to understand insulin. And to understand insulin, we need to travel to Toronto in 1922.
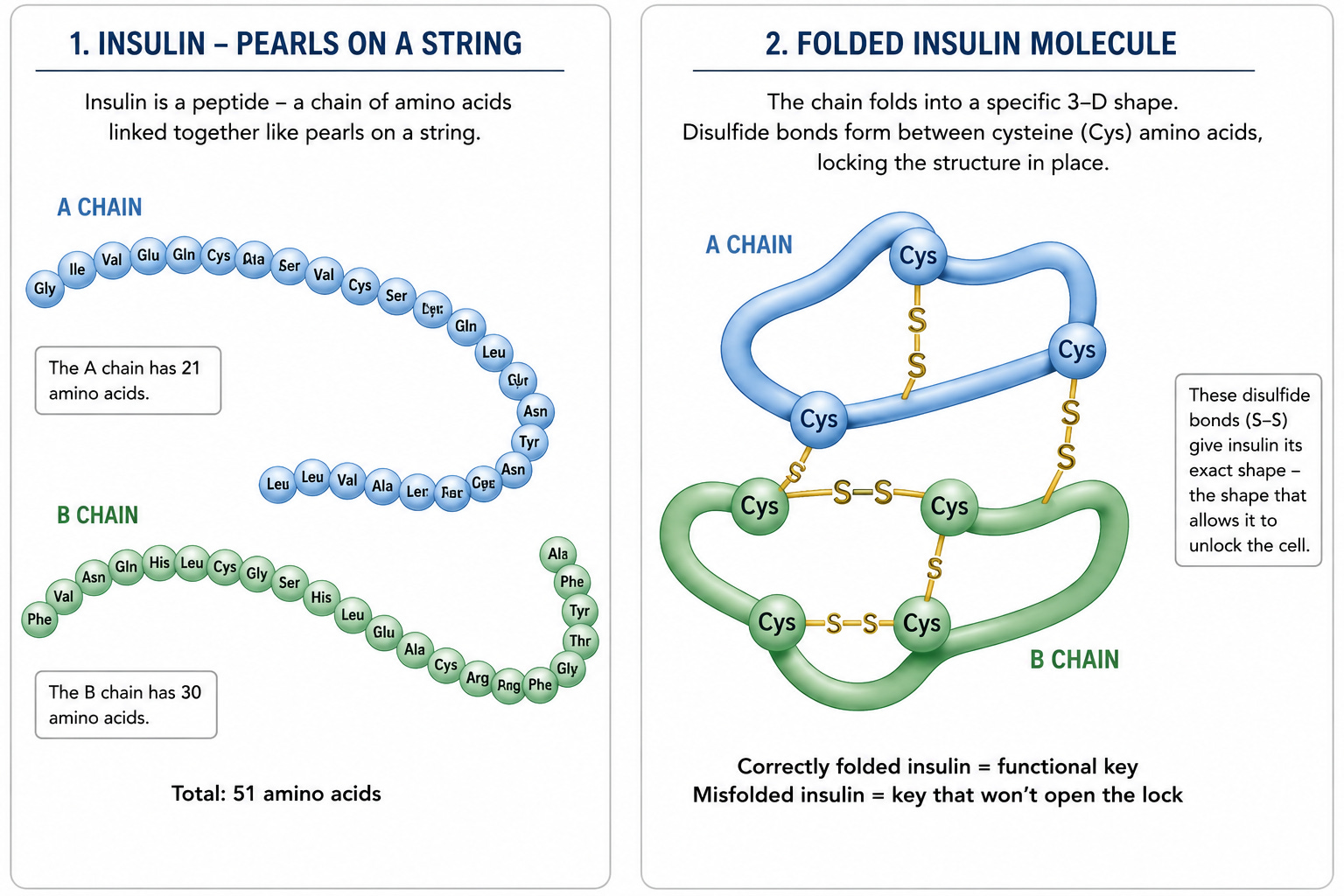
Insulin is a peptide, which means it is a chain of amino acids linked together like pearls on a necklace. Yes, a peptide is the same category of molecule that gym bros are trying to sell you out of the back of a truck. Semaglutide is a peptide. Tirzepatide—Zepbound—is a peptide. But long before social media discovered peptides, insulin was the peptide that changed medicine.
Its job is remarkably simple. Insulin acts like a key. When glucose circulates in the bloodstream, insulin tells cells to open the door and let that glucose enter. Once inside, the cell can use glucose to produce energy, repair itself, and perform all the countless little jobs that keep you alive.
Without insulin, the glucose remains trapped outside the cell. Blood sugar rises, but the cells themselves are starving. It is like standing outside a restaurant with your wallet full of cash while every door is locked. There is food everywhere, but you still cannot eat.
This is what happens in type 1 diabetes. Before insulin was discovered, children literally starved to death while surrounded by food. Their blood sugars climbed higher and higher, but the glucose could not get into the cells where it was needed. When blood sugar levels become extreme, the body begins to fail. The brain, which normally runs primarily on glucose, starts shutting down. Patients become confused, then unconscious, and eventually die.
The remarkable thing about insulin is that it is not simply a string of amino acids. Like almost every protein in the body, it must fold into a very specific three-dimensional shape. Imagine some of those amino acid pearls are tiny magnets. Certain parts of the chain attract other parts, causing the molecule to bend, twist, and fold into a very precise structure.
When the folding happens correctly, you get a functional insulin molecule—a key that fits the lock.
When the folding goes wrong, you get something else entirely.
Think of making copies of a house key. One copy is perfect and opens the front door. Another is slightly warped. It looks like a key. It feels like a key. But when you slide it into the lock, nothing happens.
Proteins are the same way.
A properly folded insulin molecule can do its job. A misfolded insulin molecule cannot.
And that matters a lot, because the cells that make insulin spend their entire lives acting like tiny factories, producing enormous quantities of this protein day after day. The harder those factories are pushed, the more opportunities there are for mistakes, misfolded proteins, and eventually trouble.
Islet of Langerhans - Not A Place to Scuba Dive
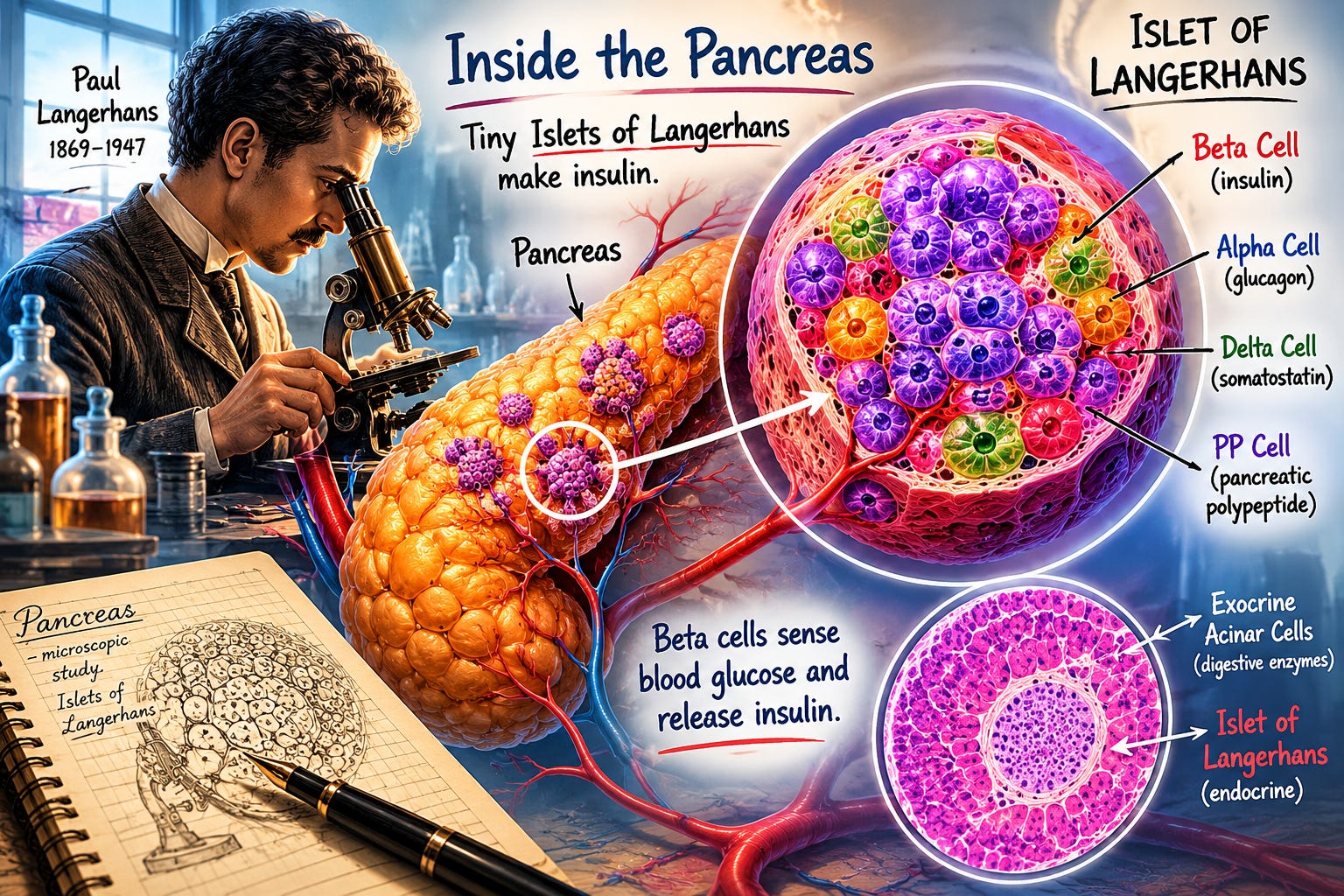
The cells that produce insulin are a very specific type of cell found in the pancreas. They are called the Islets of Langerhans, named after Paul Langerhans, a German medical student who spent a lot of time staring down a microscope. Medical students have been doing that ever since, although now they have debt and PowerPoint.
These cells have one primary job: make insulin when the body needs insulin.
Sometimes that need is obvious. Eat a large meal, especially one rich in carbohydrates, and blood glucose rises. The Islet cells respond by producing more insulin, allowing that glucose to move from the bloodstream into cells where it can be used for energy.
Not all of that glucose is burned immediately. Some of it is stored.
The liver takes glucose molecules and links them together into glycogen. Muscles do the same thing. Think of glycogen as the body’s quick-access energy account. If you suddenly decide to run, climb a hill, chase your dog, or flee a bad lecture on nutrition, glycogen can be rapidly broken apart and converted back into glucose.
That is important, because glycogen is easy to mobilize.
Fat is not.
Fat is wonderful for long-term energy storage. If human beings were designed for surviving famines, fat is the pantry in the basement. Glycogen is the snack drawer in the kitchen. When the body needs energy right now, it reaches for glycogen first.
Remember that. The liver and glycogen will become important characters later in this story.
But first, let’s go back to insulin.
In type 1 diabetes, sometimes called juvenile diabetes, the story is very different. In these patients, an autoimmune process destroys the Islet cells. We think viral infections may trigger this process in genetically susceptible individuals. By the time these children come to medical attention, the cells that produce insulin are largely gone.
No insulin.
No backup plan.
No second chance.
Without insulin, glucose remains trapped in the bloodstream, while the cells starve. Children become tired. They lose weight despite eating. They drink enormous amounts of water, because the kidneys desperately try to flush excess glucose out of the body. They urinate constantly. Parents often describe a child who seems exhausted, thirsty, and somehow not themselves.
When they present with type 1 diabetes, the game is essentially over for those Islet cells. The factory has been destroyed. If we do not replace insulin, they die.
That is why the discovery of insulin was one of the great miracles of modern medicine.
Before insulin, physicians could diagnose type 1 diabetes. They could not treat it.
Children were often placed on starvation diets to prolong life for a few months. Parents watched their children waste away, while doctors watched helplessly.
Then along came Frederick Banting and Charles Best. And medicine changed forever.
The idea of insulin was not new.
Scientists already suspected the pancreas produced some mysterious substance that controlled blood sugar. They knew that removing the pancreas from animals caused diabetes. They knew that something coming from the pancreas was essential for life.
The problem was not the theory. The problem was getting the stuff.
The pancreas is a messy organ. Most of it is devoted to making digestive enzymes powerful enough to dissolve food. Mixed among those enzyme-producing cells are tiny islands of hormone-producing cells—the Islets of Langerhans. Somewhere inside those tiny islands was the substance physicians desperately wanted.
Frederick Banting was not trying to invent a new hormone. He was trying to isolate one that nature had already invented.
Working with Charles Best in Toronto, Banting began extracting material from animal pancreases, hoping to separate the life-saving substance from the digestive enzymes that contaminated it. The work was tedious. The extracts were crude. The science was messy. Most breakthroughs look much better in history books than they do while they are happening.
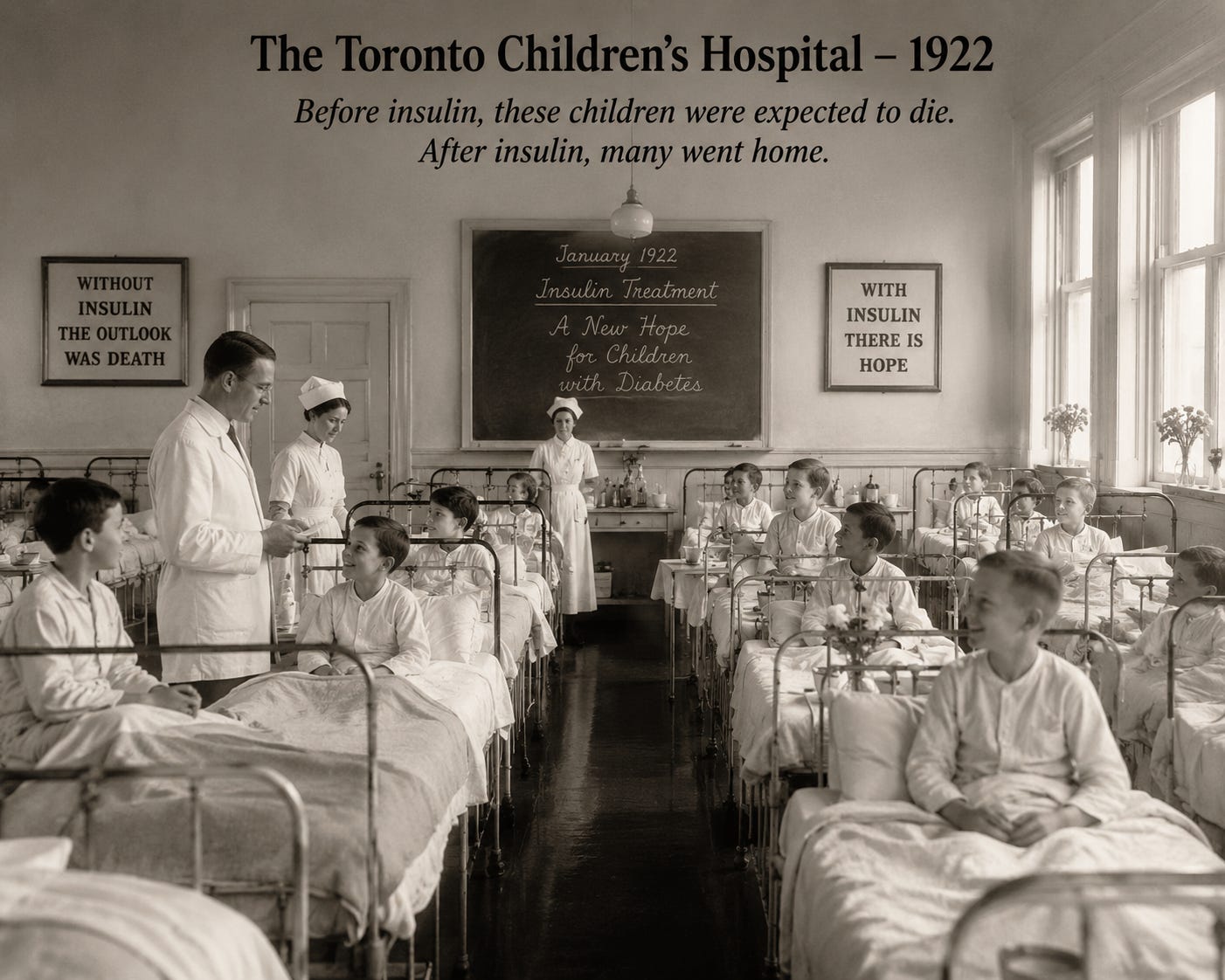
In January 1922, they treated Leonard Thompson, a fourteen-year-old boy dying of diabetes. Before insulin, children like Leonard had only one treatment available: starvation. Physicians would place them on semi-starvation diets, hoping to prolong life for a few months. Everybody knew how the story ended.
The first injection was disappointing. The extract was too impure.
Then biochemist James Collip improved the purification process.
A second injection was given.
This time it worked.
Blood sugars fell. Ketones disappeared. The boy improved.
Word spread quickly.
Soon insulin was being given to children throughout Toronto. Physicians who had spent years watching children waste away suddenly saw them sit up in bed, regain strength, begin eating, talking, laughing, and returning to life. One physician described the transformation as miraculous. Another compared it to watching the dead rise.
It is difficult for us to appreciate what that must have felt like.
Today, insulin is so common that it is easy to forget that before 1922. A diagnosis of type 1 diabetes was essentially a death sentence. Then, almost overnight, it wasn’t.
Few discoveries in medicine have changed the fate of so many people so quickly. The Nobel Prize followed in 1923. Banting was only thirty-two years old, one of the youngest Nobel laureates in history. He shared his prize money with Charles Best because he believed his young collaborator deserved equal credit.
The remarkable thing is that even after insulin was discovered, physicians still didn’t fully understand diabetes.
They had found the key. We still didn’t understand the lock.
History likes heroes, so we remember Banting and Best. What physicians remembered was something else. They remembered walking into silent wards, and finding children sitting up, talking, laughing, and asking for food. The miracle wasn't one child. It was an entire ward returning to life.
The Little Factory That Could
So if Type 1 diabetes is a disease where the factory has been destroyed, what exactly is Type 2 diabetes? For years, we thought we knew the answer. Its rise has paralleled the rise in obesity, and that is hardly surprising. What surprises many people is not finding someone with obesity and type 2 diabetes. The surprise is finding someone who is obese and doesn’t have it.
We know that the Islet cells in the pancreas produce insulin, and we know that people with type 2 diabetes require more insulin than normal. The most common reason is simple: excess calories. Those calories can come from sugar, bread, pasta, steak, butter, or olive oil. The body doesn’t care whether the excess energy arrived wearing a candy wrapper or a cowboy hat. Excess calories require more storage, more processing, and ultimately more insulin.
As more insulin is required, the cells of the body become somewhat resistant to insulin’s effects. That means the pancreas has to produce even more insulin to accomplish the same task. Think of it this way: if insulin is the key that unlocks the cell, eventually the lock becomes a little sticky. The key still works, but you need more effort to open the door.
Now let’s go back to our Islet cells.
Imagine a cardboard box factory. Every day the factory makes boxes. The boxes are folded, inspected, stacked, and shipped out. Life is good.
Then Amazon arrives. Suddenly everyone wants more boxes.
The factory ramps up production. More workers. More shifts. More pressure. Most boxes are assembled correctly, but some are folded improperly. Those defective boxes don’t get shipped. Instead, they get tossed into a corner where the factory can take them apart and recycle them.
At first, that works fine. But demand keeps increasing. More boxes are made. More mistakes occur.
Soon, the corner of the factory is piled high, with defective boxes waiting to be broken down and recycled. Eventually, there are so many bad boxes that the factory cannot function efficiently anymore.
Something similar happens inside the beta cell.
As insulin production increases, more proteins must be folded correctly. Most are. Some aren’t. Those misfolded proteins accumulate inside the cell and create stress on the cellular machinery. The cell activates emergency cleanup systems, attempting to break down the defective proteins and restore order.
For a while, the cell keeps up. Then it doesn’t.
The beta cell becomes dysfunctional. It stops producing insulin efficiently. In some cases, it essentially goes on strike, shutting down production while trying to clean up the mess. In other cases, the stress becomes so severe that the cell dies and the body removes it entirely.
The remarkable thing is that we cannot see any of this happening. Patients don’t feel a beta cell struggling. They don’t feel a protein misfold. Nor do they feel the cellular cleanup crews working overtime. That process uses an inflammatory pathway.
What we see instead is blood sugar slowly creeping upward over years. By the time the diagnosis of type 2 diabetes is made, studies suggest roughly half of beta-cell function has already been lost, and many insulin-producing cells are gone altogether.
Some cells are dead. Others are not functioning because they “are exhausted.” Kind of like my teenager after school, who stops doing work and finds a video game. Those cells are clogged with the cellular equivalent of unfinished paperwork.
The remaining cells simply work harder. That is why type 2 diabetes often progresses quietly for years before anyone notices.
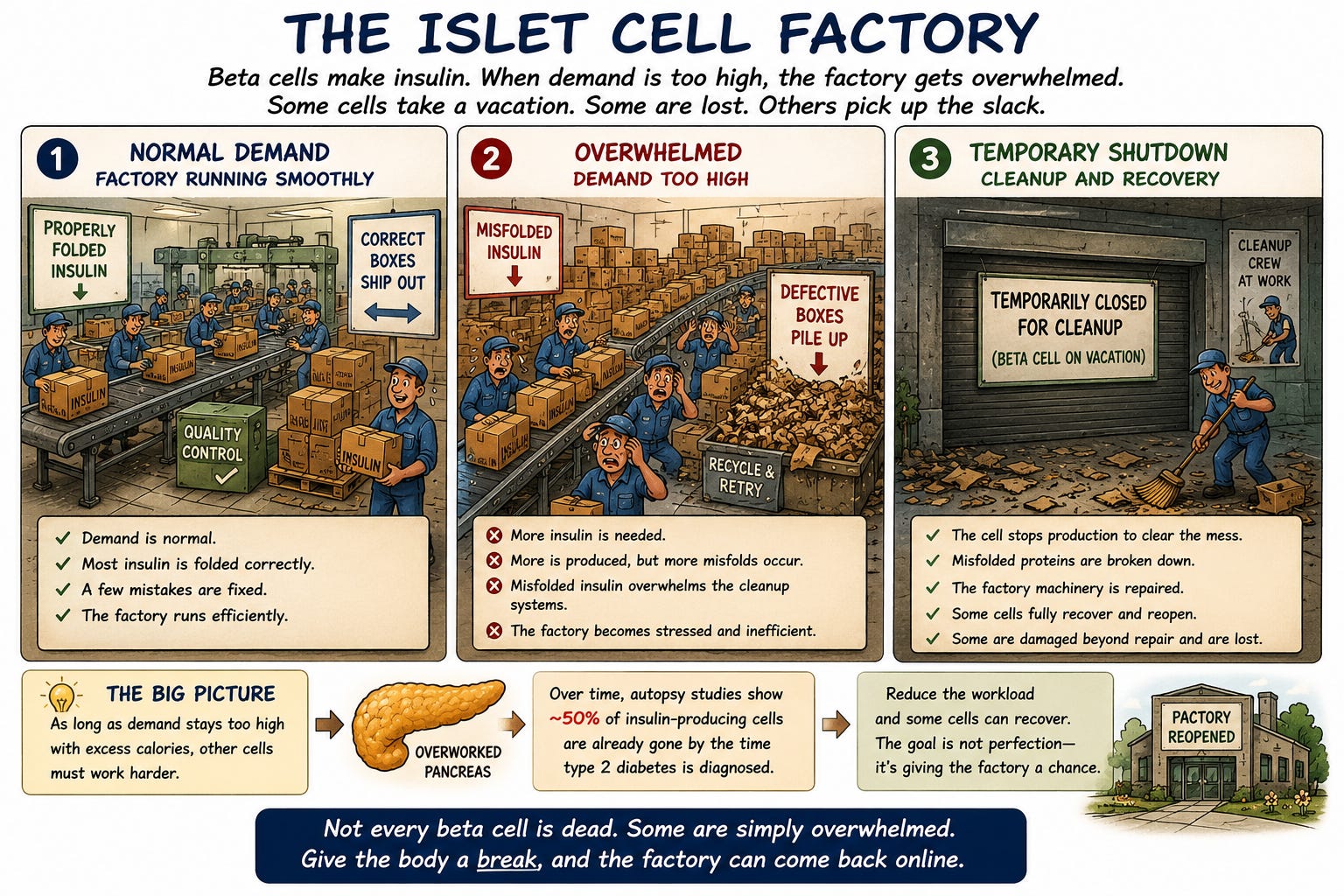
And it raises an important question: if some of those cells are not dead, but merely exhausted, what happens if we can reduce the workload and give them a chance to recover?
So where does that leave us?
We began with a mystery. Why did my patients stop needing insulin before they lost enough weight to explain it? We followed the story from the hospital ward to Toronto, from Banting and Best to the Islets of Langerhans, from insulin itself to the tiny cellular factories that spend their lives trying to produce enough of it.
Along the way, we learned something important. Type 2 diabetes is not simply a disease of high blood sugar. Blood sugar is what we measure. It is not the disease itself.
The real story is happening inside cells. It is happening inside the pancreas. It is happening long before a patient ever receives a diagnosis. By the time type 2 diabetes is recognized, many of the cells responsible for producing insulin have already struggled for years. Some have recovered. Some are exhausted. Some are gone forever.
But that still doesn’t answer the question that started this story. Why did those patients improve before they lost the weight? How could a pancreas that appeared to be failing suddenly begin working better? And what does the liver have to do with any of this?
In Part Two, we’ll follow the next clue in the mystery. We’ll meet the organ that may be doing more to drive type 2 diabetes than most people realize. We’ll look at Roy Taylor’s Twin Cycle Hypothesis, why fasting sometimes works, why low-carb advocates are seeing something real, but not the entire picture, and why the Mediterranean diet may be one of the most effective long-term treatments we have.
Most importantly, we’ll return to the modern mystery: why GLP-1 medications appear to improve diabetes faster than weight loss alone should allow.
Because the pancreas got the message before the scale did.
And we’re finally starting to understand why.
Thank you for explaining this process.
Thank you for this very informative explanation of diabetes.