

The Diabetes Mystery: Part Two
The Liver Did It

At the end of Part One, we left our beta cells in trouble. Some were dead. Others were exhausted. They were clogged with the cellular equivalent of unfinished paperwork, misfolded proteins piling up inside the cell like defective cardboard boxes stacked in the corner of an overworked factory. Production slowed. Some factories shut down for cleanup. Some never reopened.
The question is what caused all this in the first place. What made those little insulin factories work so hard that they eventually became overwhelmed? If you spend enough time on social media, you already know the list of suspects. Sugar. Fat. Seed oils. Carbohydrates. Your grandmother’s dinner rolls. You’ve seen the social media wrestling matches, as people swear they stopped sugar and their diabetes disappeared. Somewhere there is an influencer explaining that the answer involves sunlight, grounding, beef tallow, and possibly the position of Jupiter.
The stories all follow a familiar pattern. Someone gives up sugar. Someone else gives up carbohydrates. Another person starts eating nothing but steak. Someone discovers oat groats and declares civilization saved. Their blood sugars improve. Their weight comes down. They claim victory and then assume they have discovered the universal answer for everyone else.
The trouble is that every one of these suspects has at least a little evidence against them. Sugar certainly looks guilty. Excess calories are clearly involved. Genetics matter. Activity matters. Stress matters. The problem is that none of them completely explain the mystery that bothered me when I was taking care of bariatric (weight loss surgery) patients.
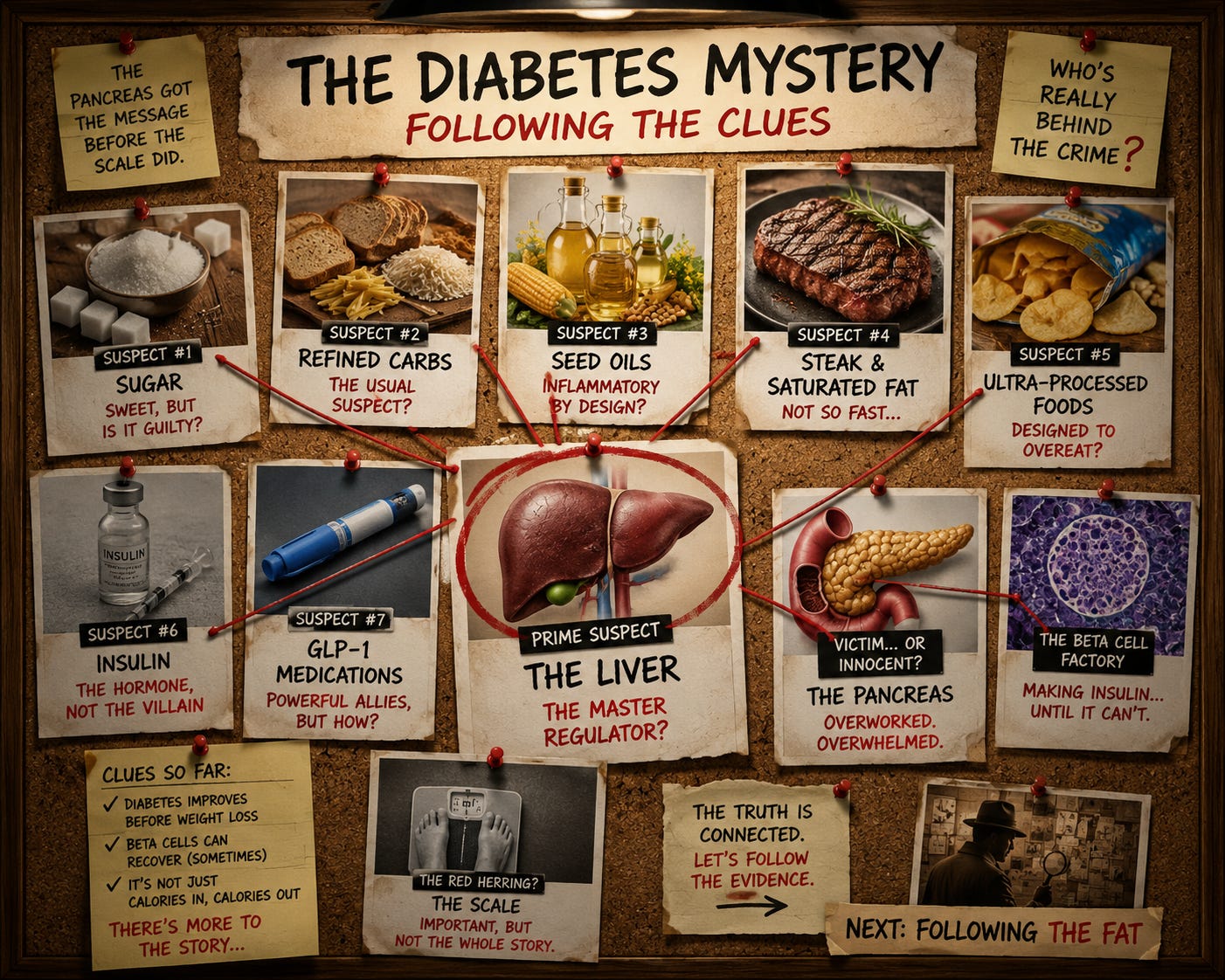
Those patients improved before they lost enough weight to explain it.
The pancreas was behaving differently. Blood sugars improved. Insulin requirements dropped. Yet the scale had barely moved. If the pancreas was the struggling factory, somebody was sending it all those work orders. Somebody was demanding more and more insulin. Somebody was creating the environment that eventually overwhelmed those cells.
To understand modern type 2 diabetes, we need to leave Toronto, leave the pancreas for a moment, and follow the clues to another organ. As it turns out, the pancreas wasn’t acting alone. It had an accomplice, and, like many accomplices in detective stories, it had been standing in plain sight the entire time.
The liver.
Now before every hepatologist writes me an angry email, let me be clear. The liver is one of the most remarkable organs in the human body. It stores energy, detoxifies chemicals, manufactures proteins, regulates hormones, and generally works harder than most of us. But like many hardworking employees, when it becomes overwhelmed, it starts making mistakes.
The Pâté Is Not a Party
The liver is one of the great storage organs of the body. Earlier, I described glycogen as the snack drawer in the kitchen. If glycogen is the snack drawer, then the liver is the person responsible for stocking it.
When blood sugar rises after a meal, insulin tells the liver to take some of that glucose and store it as glycogen. Glycogen is simply glucose linked together into long chains, a form of energy that can be quickly broken apart when you need it. If you suddenly decide to run, climb a flight of stairs, chase your dog, or flee a bad lecture on nutrition, glycogen can be mobilized quickly.
That is what the liver is supposed to do.
But like the muscle cells and fat cells we discussed earlier, the liver can also become resistant to insulin. At first, this doesn’t seem like a major problem. The pancreas simply produces more insulin. Then more. Then more still. The blood sugars often remain normal, which is one reason type 2 diabetes can hide in plain sight for years.
Eventually, however, the liver begins changing its behavior.
Instead of efficiently storing glucose as glycogen, the liver increasingly converts excess energy into fat. At first, the fat accumulates inside the liver itself. This condition, called fatty liver disease, has become extraordinarily common. For some people, it remains relatively silent. For others, it progresses to inflammation, scarring, cirrhosis, liver failure, and eventually transplantation.
If you’re a goose in southwestern France, all that liver fat may eventually become pâté. If you’re a human, it becomes a referral to a hepatologist. One is served with toast points. The other usually comes with bad news.
But for our diabetes story, another problem emerges.
The liver does not simply store fat.
It exports it.
Warehouses do not like being overfilled, and neither do livers. Once the shelves are full, inventory starts leaving the building, whether you intended it to or not. The liver begins packaging fat into triglyceride-rich particles called VLDL, and sending them out into circulation. Some of that fat ends up in muscle. Some ends up in fat tissue. Some eventually reach the pancreas itself.
At the same time, the increasingly fatty liver becomes less responsive to insulin. Insulin is supposed to tell the liver to stop releasing glucose when enough is already present in the bloodstream. The liver begins ignoring that message. Fasting blood sugars rise slightly. Not enough for a diagnosis. Not enough for a patient to notice. Just enough for the pancreas to notice.
And the pancreas responds exactly the way it always has.
It produces more insulin.
For years, that strategy works. Blood sugars remain normal. Physicians are reassured. Patients are reassured. Meanwhile, inside the pancreas, the factory is running longer hours, adding extra shifts, and asking the cleanup crews to work overtime.
The VLDL particles create another problem, one that takes us from diabetes into cardiovascular disease. These particles are not simply little fat delivery trucks. Each VLDL (cholesterol carrying particle) carries an ApoB molecule. As the liver exports more VLDL, the number of ApoB-containing particles circulating through the bloodstream increases. Many of those VLDL particles will eventually be remodeled into LDL particles, but from the standpoint of the artery wall, that distinction is less important than people think. The artery sees ApoB-containing particles, and ApoB-containing particles drive atherosclerosis.
This is one reason type 2 diabetes and cardiovascular disease travel so often together. The liver is not merely creating a problem for the pancreas. It simultaneously increases the number of particles capable of entering the artery wall. The pancreas notices the increased demand. The arteries pay the price.
Now the pancreas has two problems instead of one.
The first is that the rest of the body is becoming more resistant to insulin, which means every tissue demands more of it. The second is that the pancreas is increasingly exposed to the very fatty acids exported from the liver. Those fatty acids, particularly one called palmitate, produced by the liver during de novo lipogenesis, do more than simply sit there. They impair insulin secretion, increase cellular stress, and make it harder for the beta cells to do their jobs.
In other words, the liver is not simply sending pollution downstream.
It is increasing demand, while simultaneously making production harder.
If you were running a factory, it would be like receiving larger and larger orders every week, while somebody slowly filled the machinery with dust. The workers are asked to produce more product with equipment that works a little worse every month. For a while, they compensate. Then they begin making mistakes. Then the cleanup crews fall behind. Then production begins to suffer.
This was the observation Roy Taylor helped put together. The liver and the pancreas were not separate stories. They were feeding each other. More liver fat led to more insulin resistance, more fat export, and more stress on the pancreas. A more stressed pancreas produced more insulin. Higher insulin levels stimulated the liver to create and store even more fat. Around and around the cycle went.
Taylor called it the Twin Cycle Hypothesis.
I still think of it as two factories making each other’s problems worse.
The reason this mattered is that Taylor made a prediction. If the cycle was real, then interrupting it should reverse the process. Reduce liver fat, reduce pancreatic fat, reduce insulin demand, and some exhausted beta cells should begin functioning again.
That prediction turned out to be correct.
And suddenly, the mystery of bariatric surgery begins to look very different. Maybe those beta cells weren’t magically recovering. Maybe, for the first time in years, somebody had stopped piling new work orders on the manager’s desk.
Continuous Glucose Monitors and Weight Loss Surgery
About this time, the continuous glucose monitor companies began making the rounds.
If you’ve never met a medical device representative, they are among the most optimistic people on Earth. They can look at a surgeon who has been awake since four in the morning, is covered in coffee stains, has dictated thirty notes, and somehow conclude that what he needs in his life is another device.
In this case, they were probably right.
The pitch was straightforward. Put this little sensor on the patient, and instead of getting a handful of blood sugar measurements each day, you can see everything. Every rise. Every fall. Every spike after a meal. Every low blood sugar at two in the morning. No guessing. No relying on patient memory. Just data.
Now I love data.
I became interested in cell biology because of data. I spent years studying viruses because of data. One of my favorite phrases is that science is delighted to be wrong, because when we are wrong, nature usually has a more elegant explanation than the one we invented.
So I thought the glucose monitors were a terrific idea. More importantly, I thought they were finally going to explain what I was missing.
By this point, I had patients who were no longer taking diabetes medications. I had stopped routinely restarting those medications after surgery because of the occasional emergency room visit from patients whose blood sugar had dropped too low. The nurses rarely called for insulin coverage. The glucose logs looked good.
Frankly, they looked too good.
I had spent enough years caring for diabetic patients to be suspicious of anything that looked too good. The nurses rarely called for insulin coverage. Patients returned to clinic reporting normal blood sugars. They weren’t refilling medications. The emergency room visits from low blood sugars had already convinced me to stop automatically restarting diabetes medications after surgery.
Yet I remained convinced there was something I wasn’t seeing.
The CGM would reveal the truth.
Then we started putting them on patients.
These were not “free” because I liked data. Patients paid for them out of pocket. They paid for them, because I told them we didn’t want to miss worsening diabetes or medication adjustments. They trusted me. Looking back, some early monitors cost more than my monthly car payment.
Which only increased my determination to find what I thought I was missing
The CGM would reveal the truth. Then we started putting them on patients. Now these were not “free” because I like data. Patients paid for these, out of pocket. They paid for them, because I told them we didn’t want to miss them needing medication. They believed me, and the price of the early monitors was more than my car payment.
Before surgery, the graphs looked exactly the way you would expect. Blood sugar climbed after meals. Medications pushed it back down. Sometimes it went too low. The patient felt shaky and miserable, drank orange juice, ate crackers, or grabbed whatever carbohydrate was within reach, and then the blood sugar shot back up again.
The graph looked less like a smooth metabolic process and more like a seismograph during a California earthquake. You could practically hear the pancreas screaming.
Then the patient had surgery. I expected improvement. Everyone expected improvement. What I didn’t expect was boredom. The curves flattened. The dramatic swings disappeared. The graphs became boring. And in medicine, boring is beautiful.
The blood sugars weren’t perfect every minute of every day, because human beings are involved and human beings have a remarkable ability to surprise physicians. But the pattern was unmistakable. The chaos was gone. The highs were lower. The lows were less common. The wild oscillations that had characterized diabetes seemed to settle down with surprising speed.
The device I thought would prove my patients wrong instead proved them right.
That is not always a comfortable moment in medicine.
Physicians like to think we are objective observers, but we carry our own assumptions around just like everyone else. I assumed there were blood sugar excursions hiding between measurements. I assumed the diabetes was not improving as quickly as it appeared. I assumed the scale would eventually explain everything.
The CGM quietly disagreed.
Day after day, patient after patient, it showed the same thing. Blood sugars were normalizing long before the weight loss story should have reached that chapter.
The pancreas had gotten the message.
The scale had not.
Now, when something doesn’t fit the model, you have two choices. You can ignore it and defend the model, which is popular on social media. Or you can assume the observation is trying to teach you something.
Fortunately, medicine eventually found people willing to ask the next question. If the pancreas was improving before the weight loss arrived, what exactly was changing first?
What elegant story was mother nature trying to tell me?
The Lives of a Cell, a Beta Cell
The answer, it turned out, was both simpler and more complicated than I expected.
One thing I noticed over the years was that not every patient responded the same way. That should not be surprising, but it turned out to be important.
Most of my patients were relatively young. Many had been diagnosed only a few years earlier. They were developing diabetes, not carrying it around like an old suitcase for twenty years. Those patients often had dramatic improvements. Medications disappeared. Blood sugars normalized. Some looked as though they had left diabetes behind entirely.
Other patients improved, but not as dramatically.
The difference was often time.
The longer a patient had diabetes, the harder it became to achieve the same degree of recovery. Looking back, that makes perfect sense. If you interrupt the cycle early, many exhausted beta cells are still present. They are overworked, stressed, and functioning poorly, but they are still there. Give them a chance to recover, and they often surprise you.
Wait too long, however, and the story changes. Some cells do not recover, because some cells are gone.
You can give the remaining workers a vacation. You can reduce the workload. You can clean up the factory. But if half the workforce retired ten years ago, production will never return to where it once was.
That observation became one of the strongest evidence that we were not witnessing a miracle. We simply found that mother nature had left us an egg. The earlier the intervention, the more cells remained available to recover.
The longer the disease had been present, cells limited, the more recovery already lost.
For this group of patients, not all the islet cells were dead. Some were exhausted, overworked, and filled with misfolded proteins. In a coma, like those kids in Toronto in 1922.
What I had been watching after surgery was not a miracle. I had not performed CPR on an islet cell. I had rearranged the plumbing.
Somewhere, Gene Wilder is shouting, “It’s alive!”
The remarkable thing was that the beta cells still had enough reserve capacity to recover once the workload fell. The liver didn’t need to export fat. The body required less insulin. The pancreas could finally catch its breath. The cleanup crews inside the cells could start working through the backlog. Some of those exhausted factories reopened for business.
That realization changed the way I thought about type 2 diabetes.
The old model focused almost entirely on blood sugar due to excess weight and insulin resistance. The newer model focuses on the organs producing and responding to insulin. Blood sugar is still important, but blood sugar is the smoke. The fire is happening in the liver, the pancreas, the fat tissue, and the metabolic machinery connecting them.
I must admit there was one casualty.
The continuous glucose monitor salespeople.
Once I became convinced that most postoperative patients were doing well, I stopped recommending CGMs nearly as often. They had served their purpose. The devices I thought would uncover hidden problems had instead helped confirm that recovery was occurring much faster than I had imagined.
The important lesson is not that surgery is magical (those are the surgeon’s hands). The important lesson is that the beta cell is dynamic.
Beta cells probably have a limited lifetime, a Hayflick limit. But unlike muscles, more work does not make the cell live longer. Instead, it will struggle, and over the years, when it cannot clean out the waste material, that cell will die, and the body will replace it with scar tissue. But if you give it a chance to recover, give it a break, many of them respond beautifully.
That raises an obvious question.
If surgery works because it interrupts the cycle, reduces liver fat, lowers insulin demand, and allows beta cells to recover, then do we need surgery to accomplish those goals?
As it turns out, not always.
And that brings us to fasting, low-carbohydrate diets, Mediterranean diets, and eventually GLP-1 medications. Because once we understood the mechanism, we could begin asking a different question.
Not whether the cycle could be interrupted.
But how. And this brings us to the stories of diets, exercise, and GLP-1.
Fasting, Diets, and the hungry cell
Once you understand the twin cycles, many arguments in nutrition suddenly become less interesting.
For decades, we have searched for dietary solutions to diabetes. That should not surprise anyone. Before insulin, diet was the only treatment for type 1 diabetes. It was not a successful treatment, but it was all physicians had. Then Banting, Best, and insulin arrived, and suddenly children who would have died could live.
Type 2 diabetes was a different disease entirely.
We had medications, of course. Metformin remains one of the great drugs in medicine. Eventually, we added sulfonylureas, TZDs, DPP-4 inhibitors, SGLT2 inhibitors, insulin, and a growing alphabet soup of therapies. But dietary interventions never disappeared, because, unlike type 1 diabetes, food was clearly part of the story.
One of the more influential modern approaches came from Jason Fung. Fung took patients with advanced type 2 diabetes, encouraged fasting, reduced carbohydrate intake, and reported something remarkable. Patients lost weight. Blood sugars improved. Medications were reduced. Some patients achieved remission of diabetes.
At the time, people argued endlessly about whether fasting worked because of insulin, carbohydrates, ketosis, autophagy, ancient evolutionary pathways, or some other mechanism. Looking back, the answer appears both simpler and more interesting.
Fasting reduced the workload.
When patients stop eating for prolonged periods, glycogen stores are used. Liver fat begins to decline. Less insulin is required. The pancreas gets a break. Not the dramatic interruption produced by bariatric surgery, but an interruption nonetheless. The factory receives fewer work orders.
Low-carbohydrate diets often produce similar results. The advocates usually identify sugar as the villain. Sometimes carbohydrates become the villain. Occasionally, entire food groups are marched before a nutritional firing squad. Yet many patients lose weight, improve insulin sensitivity, reduce liver fat, and improve blood sugar control.
The more extreme carnivore versions often produce the same early story. Weight falls. Blood sugar improves. Diabetes improves. The mistake occurs when the observation is mistaken for proof of the explanation. Improvement in diabetes does not prove that carbohydrates caused diabetes, but improvement after surgery proves that stapling a stomach cures pancreatic disease.
What matters is that the metabolic workload has been reduced.
The Mediterranean diet arrives at many of the same destinations by a different road. It does not eliminate carbohydrates. It does not require ketosis. It does not require anyone to pretend vegetables are optional. Yet study after study shows reductions in diabetes, cardiovascular disease, and mortality. Patients often lose weight. They eat fewer calories without spending every waking moment thinking about calories. Liver fat declines. Insulin sensitivity improves.
In light of the biology, none of this should be surprising.
The body does not care whether you arrived there through fasting, carbohydrate restriction, Mediterranean eating, calorie reduction, exercise, or surgery. What matters is whether the liver accumulates fat or loses it, whether insulin demand is rising or falling, and whether the pancreas is being asked to work overtime.
The problem is not finding a diet that works. Most diets work. The problem is finding a diet that continues to work after the enthusiasm fades. The ice cream diet sounds great until you are on the second week and find that you have no interest in ice cream at all.
Exercise deserves special mention, because it works through several pathways simultaneously. It improves insulin sensitivity, burns glycogen, preserves muscle mass, and reduces the burden on the pancreas. If exercise were a medication, every physician in America would prescribe it. The problem is not the biology. The problem is adherence.
I know this because I owned a Peloton for two years.
I even used it once.
Yet here I am at sixty-nine, suddenly excited about yoga—I’ve been doing it for four years now—and trying to learn acrobatic planks. The lesson is not that yoga is superior to cycling. The lesson is that the best exercise program is the one you will actually do next Tuesday.
This is one reason exercise improves diabetes, even when weight loss is modest. The muscles become better customers. They take glucose more efficiently, require less insulin, and help reduce the burden placed on the pancreas. In our warehouse analogy, exercise does something diets often struggle to do: it empties the shelves while simultaneously creating room for the next shipment.
Most people know they should exercise. Most people even intend to exercise. Then life happens. Children happen. Jobs happen. Travel happens. Netflix happens. The challenge has never been proving that exercise works. The challenge has always been convincing human beings to keep doing it long enough for the benefits to accumulate.
And that turns out to be true for almost every intervention in diabetes.
This is where nutrition collides with human nature. Some people become loyal followers of Weight Watchers. Others become evangelists for low-carbohydrate eating. Others discover Mediterranean eating and never look back. A few become convinced that mankind evolved exclusively to consume ribeye steaks while contemplating mammoths.
People are wonderfully diverse.
Human nature is remarkably consistent.
The uncomfortable reality is that sustained remission through dietary intervention alone is uncommon. We hear the testimonials because success stories are interesting. We rarely hear from the far larger group of people who quietly regained weight, saw diabetes return, and moved on with their lives.
This is one reason bariatric surgery remained so important for so long. Study after study demonstrated rates of diabetes remission that dietary interventions struggled to match, particularly over the long term. Surgery did not work because it was magical. It worked because it reliably interrupted the cycle. Unlike most diets, patients could not simply quit it on a Tuesday afternoon after a stressful day.
But science had another surprise waiting.
A new class of medications appeared capable of producing many of the same biological effects without an operating room.
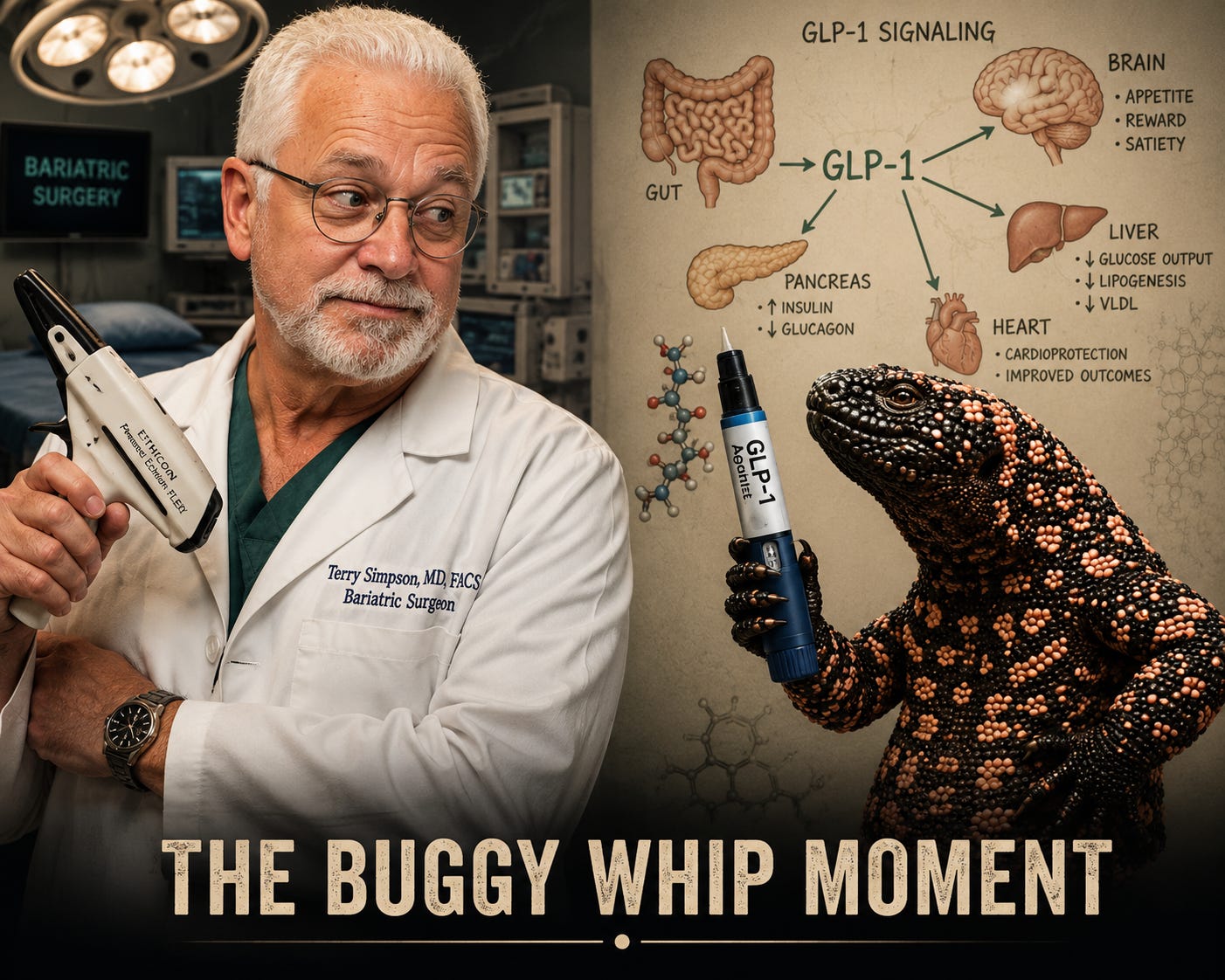
And suddenly bariatric surgeons began looking like manufacturers of buggy whips watching the first automobile drive down the street.
The Drug That Shouldn’t Work This Well
Imagine a drug that is remarkably close to bariatric surgery in terms of weight loss.
Now imagine the same drug lowers blood sugar, improves fatty liver disease, reduces cardiovascular events, improves kidney disease, quiets food cravings, and appears to help preserve some of the very beta cells we have spent this entire article discussing.
If I had told you twenty years ago that such a drug was coming, most physicians would have laughed. Many surgeons would have laughed harder.
For most of my career, the most effective treatment for severe obesity and type 2 diabetes involved anesthesia, staplers, operating rooms, and a patient willing to let me rearrange their plumbing. The results were often remarkable. Patients lost weight. Blood sugars improved. Medications disappeared. Fatty livers improved. Some patients achieved long-term remission of diabetes.
When weight loss surgery was compared to any lifestyle or diet, weight loss surgery won that argument again and again. In multiple papers, but here was a drug that did what we couldn’t do - people would take a drug, and less than 2 percent of people eligible for surgery would choose to have an operation.
What fascinated me most, however, was never the weight loss. It was the timing. The diabetes often improved before the weight loss could explain it.
That observation bothered me for years. The hospital records showed it. The glucose logs showed it. The continuous glucose monitors showed it. The pancreas seemed to get the message before the scale did.
Then along came the GLP-1 medications.
The first of these drugs reached the market in 2005. Exenatide was developed from a peptide discovered in the saliva of the Gila monster, which proves that Mother Nature is far more creative than most pharmaceutical companies. The early drugs effects were modest by modern standards. They improved blood sugar control. Patients lost some weight. Insulin sensitivity improved. Beta-cell function appeared to improve.
Interesting, but not revolutionary. The push for better drugs is driven by the marketplace, and weight loss and better diabetic control led to learning more about the GLP-1 pathway, and making drugs that have more effect.
Patients were losing far more weight than expected. Blood sugars were improving more rapidly than expected. Fatty liver disease was improving. Cardiovascular risk was falling. Some patients described something physicians rarely measure and almost never discuss.
The food noise disappeared. As a bariatric surgeon, that caught my attention immediately. At first when someone said that, it was a patient who had a RNY gastric bypass, and now, on some peptide, she said her head was in a better place. I didn’t frankly believe it. But her results were clear. Then came in a patient who wanted a revision because she had regained her weight years after her RNY bypass. I decided to try her on Ozempic, and over the next six months she lost more weight than she had after her initial bypass. But here was the other key, after she gained some, she developed diabetes, something she had not had before, so the Ozempic was for that. But it did more.
Her story sounded familiar. Less food entering the system. Less liver fat, something we could see on our ultrasound. Less insulin demand. More opportunity for exhausted beta cells to recover.
In other words, many of the same biological pathways that had made surgery so effective appeared activated by a weekly injection. And instead of a complex revisional surgery, we had a weekly injection doing the same thing, and in this case better, than her RNY bypass.
What fascinated researchers was that the story did not stop at appetite.
As the studies accumulated, it became clear that GLP-1 drugs were doing far more than helping people eat less. Beta cells survived longer. Some studies suggested new beta-cell formation. Damaged beta cells appeared better able to recover. The mitochondria inside those cells—the tiny power plants responsible for producing energy—functioned better and were protected from some of the metabolic stress that accompanies diabetes.
The liver was changing too.Insulin sensitivity improved. Fatty liver disease improved. The constant export of fat from the liver slowed. The very cycle Roy Taylor had described years earlier appeared interrupted from multiple directions at once.
That was the part that caught my attention.
For years, I had watched surgery improve diabetes before the weight loss could explain it. Now I watched a medication produce many of the same effects. Not identical effects, and certainly not in every patient, but enough similarities that it became impossible to ignore.
A peptide discovered through studying the saliva of a desert lizard was influencing the pancreas, the liver, the gut, the brain, and perhaps even the survival of the very cells responsible for making insulin.
That is not a weight-loss drug, it is a metabolic drug.
And to understand why it works, we need to go back to a discovery that changed how we think about the gut itself.
Because your intestines are not simply a tube that absorbs food.
They are one of the most sophisticated endocrine organs in the human body.
